As I promised here my English translation of Chappertron’s „Rettung der Gesundheit“, Part 1.
It's been a while since my articles on autophagy & mTOR, but I would like to take this opportunity to take another look at a reply.
caloric restriction mimetics (CRM for short) and suggested that these CRMs could probably extend telomeres or even induce autophagy.In his reply, @lauch3d mentioned the term
First of all, I must confess that I had never heard of the term CRM, but in principle I was still familiar with it, because it is essentially a collective term for different strategies for preventing diseases and aging.
So maybe we should first see what CRM means.
CRM is very closely correlated with the term of CR, caloric restriction which means that the body is deprived of a certain amount of nutrients. This consequently leads to the activation of health-promoting mechanisms. Closely associated with CR is also the term DR, which describes diet restriction, which is simply a diet.
Let's start with the definition of CR & DR.
Both terms basically mean the same thing, namely the restriction of food intake, by up to 60%, thereby achieving a positive effect on health and aging [1]. Especially in the case of CR it is thereby important to prevent malnutrition.
For CRM, the whole thing looks a bit different.
According to Ingram & Roth [1], CRM describes a substance that mimics the metabolic, hormonal and physiological effects of CR. Essentially, CRM is characterized by the following mechanisms:
• Induction of stress responses
• Improve protection against stress
• Extension of life as in the case of CR
• Reduction of diseases related to aging
• Adolescent body functions should be preserved
• The whole thing has to happen without reducing the intake of food
Especially the last point is of huge importance here. CRM should enable you to continue with your life as usual, but the body works comparable a body which is de facto on a diet, but without hunger, without a JoJo effect, without nutritional plans, without discipline.
In principle, the perfect tools for our modern society:
Do I have any physical ailments? Just take some pills! If you are in a bad mood or you are not powerful enough? Simply use anabolic steroids, stimulants or neuro-enhancers! My body is not perfect? Let's get corrected by surgery! Might you get problems with a wrong lifestyle? No problem, use some CRMs and keep going as you did it before.
At first, it is important to know that the CR can definitely serve as a life-prolonging strategy. The following figure will describe this briefly.
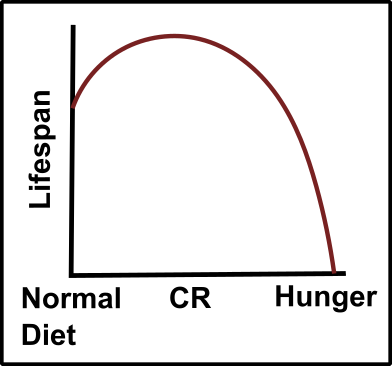
Fig.1: The lifespan under normal condition (normal diet), while doing a caloric restriction (CR) or under hunger. Made by Chapper - unrestricted use allowed
I found this conclusion in an article on this subject [2]. You can clearly see that the CR could have a positive effect on the lifespan. At a certain point, when you start to become hungry, the whole thing tips over and you get serious problems. This hunger leads to a significant reduction in lifespan and eventually death. It is therefore crucial that you listen to your body and constantly keeping an eye on your health parameters while doing something like a CR. For example, if you are constantly hungry and feeling worse, this is certainly a clear sign that you are on the outer borders of the CR (caloric restriction, not Czech Republic 😉).
It is also important to understand that in some studies these effects were not reproducible. This is a biological issue due to biological systems are complex and hard to predict.
In addition, it is important to note that these effects were primarily studied on worms, flies and mice [2]. The reason is simply their experimentally manageable lifespan, as well as the fact that it is an ethically problem to try comparable studies with humans. Nevertheless, close relatives of humans such as higher mammals like monkeys may give you a better insight. Indeed, such effects were also observable in monkeys [3]. Additionally, you can estimate a potential effect of CR by studying the personal fate of people. This is called the Methuselah effect, and occurs primarily in people who had a lower food intake or were forced to eat less due to certain circumstances (e.g., due to wars, famines or other comparable events) [4].
It should be noted: CR is a scientifically well-studied method for the potential extension of life!
But what's about CRM and which strategies belong to CRM?
Basically, the CRM requires the intake of substances or even the surgical modulation of the body [1]. The latter is, for example, the installation of a gastric band, which of course reduces food intake, simply because the saturation occurs faster. Nevertheless, such measures are associated with risks. For instance, an operation shortens your life to a certain extent. Such actions are therefore likely to be relevant only to people who fail to manage weight problems in another way. For healthy people, this is, in my opinion, not an option.
Thus, primarily only drugs, supplements and comparable substances remain in order to realize the CRM.
Such substances are, in addition to already established substances such as aspirin, metformin or fiber-rich nutrients (my personal opinion), especially substances with potential risks such as 2-deoxy-D-glucose (2-DG) and rapamycin.
We already know rapamycin from the second article on autophagy & mTOR.
Rapamycin is an antibiotic from the Easter Island (Rapa Nui), which inhibits mTOR and thereby activates autophagy. In fact, rapamycin has been extensively studied for lifespan extension and is actually the most potent drug in the field of CRMs [1]. However, rapamycin has many side effects. First, there are some fertility problems in male rodents to mention [5]. In addition, prolonged use promotes insulin resistance and other metabolic problems [1, 6, 7], as well as suppression of the immune system [8]. Just like in my autophagy articles (here, here and here), mTOR is also useful for the body. The administration of a specific substance, with a specific effect, thus leads to a cascade of problems that may end up in a plethora of nonspecific effects. It is therefore difficult to estimate how rapamycin affects in the body, even though you already know how it works on a cellular level. And rapamycin is really a potent inhibitor, probably one of the most efficient inhibitors I've ever used. A long time ago I used it in cell culture experiments, let's have a look on this Western blot:
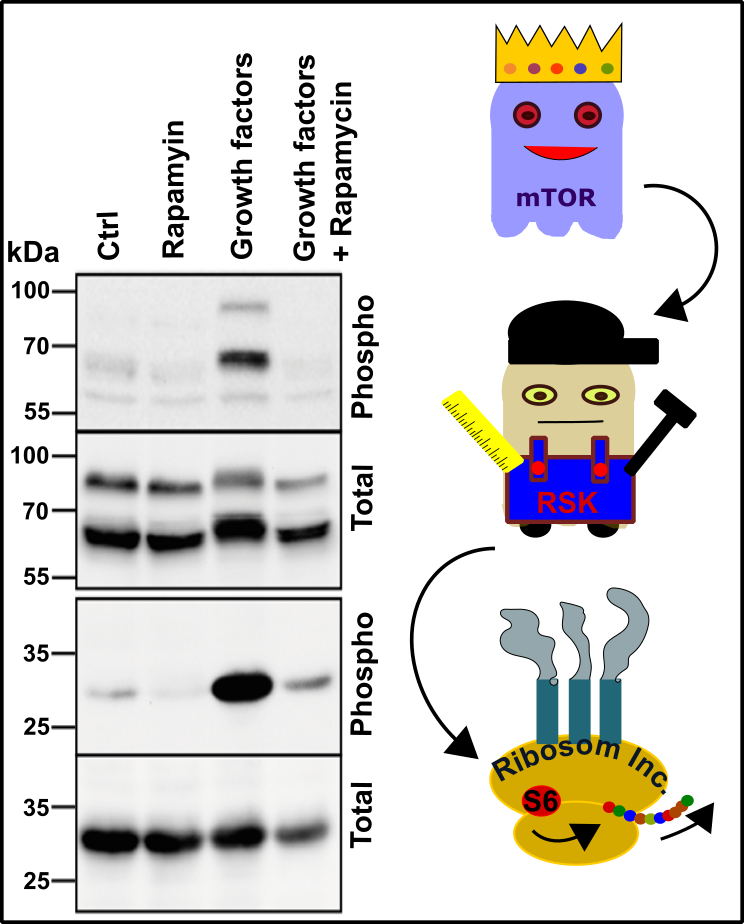
Fig.2: mTOR signaling leads to ribosomal S6 phosphorylation. Rapamycin can efficiently block the pathway which is induced by growth factors. For further details please see text. Made by Chapper - unrestricted use allowed
I used kidney cells and stimulated them with growth factors. The expected reaction, namely the phosphorylation of the ribosomal kinase RSK, was observable. This kinase then phosphorylates the ribosomal S6 protein, which is responsible for boosting protein expression. Since mTOR is the main kinase for these effects, I was able to efficiently suppress the phosphorylation of both targets by adding rapamycin, without significantly changing the total protein amount. In addition, in further experiments I could never observe (compared to other inhibitors) that rapamycin turns anything on or off except of mTOR and mTOR-related targets. Rapamycin is therefore very specific and extremely effective, even nanomolar doses show clear effects. In principle a dream!
Since 2-deoxy-D-glucose (2-DG) is also extremely reliable concerning it’s reaction in cellular metabolism and signaling, substances like this are comparable to rapamycin.
In the article on autophagy & mTOR we discussed carbohydrate metabolism. 2-DG inhibits the pathway that is at the very beginning of cellular glucose degradation, namely glycolysis. Glycolysis is a pathway through which a lot of energy can quickly be generated. If the mitochondria (which are responsible for further processing of the end product of glycolysis, pyruvate) are not able to work together with glycolysis, pyruvate is reduced to lactate and acidifies the cell and its environment. This mechanism is also partially pathological, for example in tumor cells [9]. Here, the cells rather use the so-called anaerobic glycolysis (i.e. only the branch to the pyruvate, which does not need (!) oxygen) and therefore accumulate much lactate [9]. Cancer cells thus prefer the anaerobic glycolytic degradation of glucose as a growth substrate. This mechanism, known as the Warburg effect, was proposed decades ago by the famous biochemist Otto Warburg [10], but has only recently received more attention [9].
[To prevent confusion: Glycolysis itself is an anaerobic pathway due to no oxygen is needed. The final product of glycolysis is pyruvate. This pyruvate can now either go into mitochondria with a consequent consumption of oxygen or generate lactate (=acid). No oxygen is needed in the last case. That's why I define the generation of lactate as anaerobic glycolysis. [Please note, that also under conditions with oxygen you receive acid, e.g. hydrogen carbonate.] In the literature it's often called aerobic glycolysis due to lactate is created even though oxygen is available. I personally think this is confusing. My definition is as follows:
Glycolysis with a concomitant creation of lactate = anaerobic glycolysis
Glycolysis with no creation of lactate = aerobic glycolysis
My definition is also in accordance with the definition Otto Warburg did. In the famous paper of him [10], he wrote:
The anaerobic glycolysis of the high-malignancy line 1742 was QmN2 = 60 to 80, which is virtually maximum for any and all cancer cells previously reported, including ascites cells. The anaerobic glycolysis of the low-malignancy line was, however, only one-third as great, QmN2 = 20 to 30. The average aerobic glycolysis values for the two lines were in the same order, QM02 = 30 and 10, respectively, but of lower magnitude because of the usual, pronounced Pasteur effect, greater in line 1742 than in line 2049 (QMN2 - QM02 = about 40 and 15). On the other hand, the rates of oxygen consumption were in the converse order, being smaller in line 1742 (Qo2=5 to 10) than in line 2049 (Qo2 = 10 to 15), corresponding to a greater degree of respiratory defect in line 1742.
OK!?!]
Anyway, because of the relation to glycolysis and cancer, 2-DG was one of the first and most promising CRMs [1], but a lot of problems emerged. 2-DG appeared to cause heart problems in animal experiments with rats. Which in principle is completely comprehensible, because the heart consumes the most energy in the body [11], which is why the energy-yielding pathways should work as well as possible. [Please note that heart muscle cells prefer the consumption of fatty acids [12], therefore it’s not completely clear where this effects are coming from!]
Incidentally, the assumption that the inventor of the Atkins diet ultimately died of heart problems is quite interesting in this context [13]. The Atkins diet provides for a strong shift to high-protein diet, with significant reductions in carbohydrates. It's only speculation but raises the question whether a radical low-carb diet and other strategies might eventually be very unhealthy. Check my autophagy article for more information.
As in the case of rapamycin, 2-DG is also very efficient. In the following picture you can see a measurement I did with my platelets:
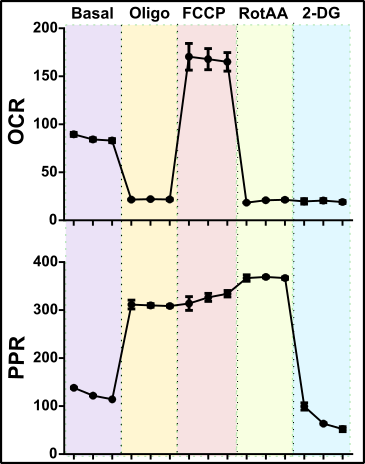
Fig.3: Chapper’s platelets in a Seahorse. For further details please see text. Made by Chapper - unrestricted use allowed
I took my blood, isolated some platelets and checked their mitochondrial and glycolytic capacity. As you can see, my platelets use the available oxygen in a high amount thus my mitochondria performing well. This can be seen by the amount of oxygen consumed, the Oxygen Consumption Rate (OCR). After inhibition of mitochondrial ATP synthase by Oligomycin (Oligo), the platelets begin to push their anaerobic glycolysis. Therefore, the platelets are generating much more acid, which is expressed by a significantly increased rate of secreted protons, the so-called Proton Production Rate (PPR).
The decoupling of the mitochondrial respiratory chain by FCCP promotes more oxygen consumption, but this is probably more about dissolved carbon dioxide as I described above. After addition of Rotenone & Antimycin A (RotAA) the mitochondria are completely inhibited. Now my platelets use almost exclusively anaerobic glycolysis, the PPR therefore increases. However, the addition of 2-DG stops this abruptly. You can see that the platelets immediately stop to secret protons (strong PPR reduction !!!). Therefore, Game Over for glycolysis!
Based on observations such as them, it was conceivable to use 2-DG to eliminate glycolysis and thus starve tumors. In fact, this has already been tried, but it turned out that in addition to the heart problems (already mentioned above), the optimal dosage is also a problem [1]. I do not know to what extent 2-DG is currently being tested or used clinically.
But one thing I know: Using 2-DG in my daily diet is not an option.
So you can probably guess that CRMs are not an easy approach to improve your health and wellbeing.
In addition to a stomach surgery, rapamycin or 2-DG there are also substances such as metformin. Metformin is a biguanide, which has been known since the late fifties according to entries at NCBI. Therefore, it is already in use for a long time. Metformin is one of the most used drugs for the treatment of diabetes mellitus type 2 (check also the article series of Scienceblocks, as well as my articles about autophagy) because of it's ability to reduce the uptake of glucose through the gastrointestinal tract or by an increase in glucose uptake by cells [14]. Thus, the blood sugar level is kept at a moderate level and unpleasant side effects are reduced. In addition, life-prolonging effects of metformin have been observed in some animal studies. In worms, for example, metformin was found to trigger an effect called mitohormesis [15]. Mitohormesis is a mechanism characterized by an increased production of reactive oxygen species (ROS) such as hydrogen peroxide. These species are not harmful in that case and promoting the activation of stress pathways which improve survival [16]. I had already mentioned this in the autophagy article when it came to the positive effects of sports. Sports in combination with vitamin supplementation is not recommended because it prevents advantageous stress pathways [17]. Similar observations were also made with 2-DG [18]. In worms it was shown that 2-DG causes oxidative stress and a longer lifespan. However, the addition of vitamin C and E prevents these effects immediately. Therefore, keep your fingers off vitamin supplementation (except perhaps Vitamin D [13]).
Alright so far!
But is it advisable to intervene prophylactically with metformin?
First of all, some side effects were observed caused by metformin, as with probably any medication. An effect often occurs after use of metformin is the so-called lactic acidosis [19]. This is the acidification of the body with lactate due to an increased rate of anaerobic glycolysis, as I already described above. In addition, one study has shown that sports have similar, if not better, effects than metformin [13, 20-22]. So if you ask me if metformin is good for you or not, all I just can say is that sports are really helpful.
But are there any other possibilities in the big wide CRM world?
A great review on the subject is certainly the article by Roth & Ingram 2014 [1]. This article lists a lot of potential CRMs. For example, there is 3-bromopyruvate, which inhibits the first step of glycolysis and is toxic to the liver and gastrointestinal tract in animals. Further, it inhibits the metabolism in the brain and in sperm cells. Or various substances that inhibit the absorption of fats or carbohydrates. For instance, chitosan, which, however, shows only minimal or no detectable clinical effects. Or orlistat which shows side effects in 36% of all cases.
After a thorough review by myself, I can conclude that many CRMs have little or no effect (or are even harmful). However, it might be primarily due to insufficient research in this field. Nevertheless, the biggest problems are probably the side effects which were documented very often.
A substance that has shown no dramatic side effects or displayed any obvious toxicity in more than 20 years of research is acarbose [23]. Possible side effects include, for example, flatulence.
What is acarbose doing?
Acarbose is a sugar, which, however, cannot be digested by human enzymes. For this reason, acarbose inhibits enzymes called hydrolases, which are responsible for carbohydrate breakdown, especially α-amylase and α-glucosidase. When starch is consumed, α-amylases, which are already present in the oral cavity, becomes active [24]. Eventually, in the intestine, both enzymes are needed to break down starch into its individual parts.
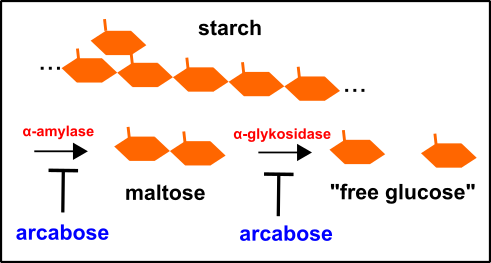
Fig.4: Enzymatic digestion of starch and the role of acarbose. Made by Chapper - unrestricted use allowed
By the action of acarbose this process is stopped, thereby reducing the amount of "free glucose". Of this reason, you feel full without energy overload or insulin secretion.
In fact, an increases in lifespan was observed in mice after administration of acarbose [23]. Unfortunately, studies show that this is primarily the case for males [25].
Other substances that are less problematic, but also need further research are trans-reseveratrol, as well as nicotinamide and spermidine (see also the autophagy articles here and here about this).
Nicotinamide is a component of the NAD and NADP, please check my articles concerning autophagy again for further details. Both substances transport (as we already know) the reduction equivalents from the nutrients in order to extract energy from them.
I do not know exactly why nicotinamide could be a possible CRM. It is conceivable, however, that a sufficient presence of redox carriers the metabolism is enabled to work more efficiently. This could be due to the extent of anaerobic glycolysis is reduced and the mitochondrial activity is elevated (the main cause of anaerobic glycolysis is a lack of oxidized NAD!). The mitochondria, in turn, are the primary source for the formation of reactive oxygen species (ROS) and thus the trigger of mitohormesis [16]. Please note, that this is solely an assumption by me.
Nicotinamide is derived from vitamin B3 and, as already mentioned elsewhere, represents a significant cofactor in the cellular metabolism. Read my articles about autophagy again, to find out more concerning sources of vitamin B3.
Spermidine is another potential candidate for CRM, which you can mainly find in cheese, soy, mushrooms, as well as various types of fruits and vegetables. Incidentally, Harzer (a special cheese from the Harz mountains in Germany) is one of the cheeses with the highest spermidine content of almost 40 mg per kg, followed by less than 30 mg per kg in Old Amsterdam, Tilsiter and Cheddar [13]. If you do not like Harzer, use the other variants.
But what is spermidine actually doing?
Spermidine primarily activates our autophagy and prolongs lifespan, at least in yeasts, flies, and worms [26, 27]. However, it has also been found in humans that there is a correlation between a long life and spermidine. The problem is that the amount of spermidine decreases with age [28, 29]. Spermidine seems to prolong life by various mechanisms, as indicated in the cited sources. Accordingly, we come back to where we have arrived so often, namely at the conclusion that a healthy lifestyle is half the battle.
Ok, I think that's enough for the moment concerning the big wide world of CRMs.
It's time for a conclusion.
In my opinion, there is, of course, a potential benefit by CRMs, but after carefully researching the literature I come to the same conclusion as in my autophagy articles. Even though that most of these (primarily) synthetic substances may have helpful effects, the side effects of them are major drawbacks. On the other hand, there are numerous other substances such as spermidine from cheese and vegetables, or nicotinamide from plants and yeasts or even a high-fiber diet, which automatically ensures that you are fed up faster, longer and healthier. In addition, there are sports or exercises, which are proven to be more effective than many diabetic medicines [13, 20-22]. Therefore, I do not see any reasonable need (unless absolutely necessity in medical terms) that a healthy person should inject something like rapamycin, 2-DG, metformin, or 3-bromopyruvate. Rather, it will hurt you than elevating your health and wellbeing.
Here are my top 3 CRMs for you:
- A balanced and healthy diet, rich in cheese and vegetables
- Sports
- If you need something synthetic, then acarbose
Well, that should be enough for now. As I said, please bear in mind that this is not a proposal of a physician. It is my personal view that I came to because of my research. In addition to the CRMs, there is of course also the CR and in particular the Intermittent fasting, which I have already mentioned in my autophagy article(s).
What remains is the big question about telomeres. I will tackle these in the next article(s) and then we can also interconnect this with autophagy & Co.
Until then, I wish you a pleasant rest Sunday and a nice start to the new week.
Cheers,
Chapper
References
All pictures were made by myself and can be used without restriction.
If you want to browse a little further, then go through this list:
- Ingram, D.K. and G.S. Roth, Glycolytic inhibition as a strategy for developing calorie restriction mimetics. Exp Gerontol, 2011. 46(2-3): p. 148-54.
- Szafranski, K. and K. Mekhail, The fine line between lifespan extension and shortening in response to caloric restriction. Nucleus, 2014. 5(1): p. 56-65.
- Fontana, L., L. Partridge, and V.D. Longo, Extending healthy life span--from yeast to humans. Science, 2010. 328(5976): p. 321-6.
- B., G., Gerontologie - Der Methusalem-Effekt. Spektrum der Wissenschaft, 2017. 2.17.
- Oliveira, P.F., C.Y. Cheng, and M.G. Alves, Emerging Role for Mammalian Target of Rapamycin in Male Fertility. Trends Endocrinol Metab, 2017. 28(3): p. 165-167.
- Blagosklonny, M.V., Once again on rapamycin-induced insulin resistance and longevity: despite of or owing to. Aging (Albany NY), 2012. 4(5): p. 350-8.
- Blagosklonny, M.V., Rapamycin-induced glucose intolerance: hunger or starvation diabetes. Cell Cycle, 2011. 10(24): p. 4217-24.
- Barlow, A.D., M.L. Nicholson, and T.P. Herbert, Evidence for rapamycin toxicity in pancreatic beta-cells and a review of the underlying molecular mechanisms. Diabetes, 2013. 62(8): p. 2674-82.
- Liberti, M.V. and J.W. Locasale, The Warburg Effect: How Does it Benefit Cancer Cells? Trends Biochem Sci, 2016. 41(3): p. 211-218.
- Warburg, O., On the origin of cancer cells. Science, 1956. 123(3191): p. 309-14.
- Roberts, S.B.D., Sai Krupa, Was unser Körpergewicht bestimmt. Spektrum der wissenschaft, 2017. 11.17: p. 12-18.
- Grynberg, A. and L. Demaison, Fatty acid oxidation in the heart. J Cardiovasc Pharmacol, 1996. 28 Suppl 1: p. S11-7.
- Kast, B., Der Ernährungskompass: Das Fazit aller wissenschaftlichen Studien zum Thema Ernährung - Mit den 12 wichtigsten Regeln der gesunden Ernährung. 2018: C. Bertelsmann Verlag.
- Wang, Y.W., et al., Metformin: a review of its potential indications. Drug Des Devel Ther, 2017. 11: p. 2421-2429.
- De Haes, W., et al., Metformin promotes lifespan through mitohormesis via the peroxiredoxin PRDX-2. Proc Natl Acad Sci U S A, 2014. 111(24): p. E2501-9.
- Ristow, M. and K. Schmeisser, Mitohormesis: Promoting Health and Lifespan by Increased Levels of Reactive Oxygen Species (ROS). Dose Response, 2014. 12(2): p. 288-341.
- Ristow, M., et al., Antioxidants prevent health-promoting effects of physical exercise in humans. Proc Natl Acad Sci U S A, 2009. 106(21): p. 8665-70.
- Schulz, T.J., et al., Glucose restriction extends Caenorhabditis elegans life span by inducing mitochondrial respiration and increasing oxidative stress. Cell Metab, 2007. 6(4): p. 280-93.
- Nasri, H. and M. Rafieian-Kopaei, Metformin: Current knowledge. J Res Med Sci, 2014. 19(7): p. 658-64.
- Stanford, K.I. and L.J. Goodyear, Exercise and type 2 diabetes: molecular mechanisms regulating glucose uptake in skeletal muscle. Adv Physiol Educ, 2014. 38(4): p. 308-14.
- Smith, A.D., et al., Physical activity and incident type 2 diabetes mellitus: a systematic review and dose-response meta-analysis of prospective cohort studies. Diabetologia, 2016. 59(12): p. 2527-2545.
- Knowler, W.C., et al., Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med, 2002. 346(6): p. 393-403.
- DiNicolantonio, J.J., J. Bhutani, and J.H. O'Keefe, Acarbose: safe and effective for lowering postprandial hyperglycaemia and improving cardiovascular outcomes. Open Heart, 2015. 2(1): p. e000327.
- Püschel, Taschenlehrbuch Biochemie. 2011: Thieme Verlagsgruppe.
- Harrison, D.E., et al., Acarbose, 17-alpha-estradiol, and nordihydroguaiaretic acid extend mouse lifespan preferentially in males. Aging Cell, 2014. 13(2): p. 273-82.
- Madeo, F., et al., Spermidine: a novel autophagy inducer and longevity elixir. Autophagy, 2010. 6(1): p. 160-2.
- Eisenberg, T., et al., Induction of autophagy by spermidine promotes longevity. Nat Cell Biol, 2009. 11(11): p. 1305-14.
- Madeo, F., et al., Spermidine in health and disease. Science, 2018. 359(6374).
- Madeo, F., et al., Spermidine delays aging in humans. Aging (Albany NY), 2018. 10(8): p. 2209-2211.
This post has been voted on by the SteemSTEM curation team and voting trail in collaboration with @utopian-io and @curie.
If you appreciate the work we are doing then consider voting all three projects for witness by selecting stem.witness, utopian-io and curie!
For additional information please join us on the SteemSTEM discord and to get to know the rest of the community!
Regarding telomeres, there's research that you can actually make them grow through diet. But I guess you might mention that in later articles of this series, which I'll read at a later date!
Hey Alex,
sorry for answering so late. I was afk the last days.
Yes, I mentioned this already in previous articles. The telomerase activity depends on the cell type. Stem cells, sperm cells and some cells of the immune system display a remaining telomerase activity the entire life.
Actually, you can promote this by diet, even though it is not completely understood thus far. I cited articles where they tried to figure out which molecular mechanisms are involved. Check this article here.
In the end, fasting is a good idea in any case!
Happy new year
Chapper
I have been semi fasting for over three months now, only drinking coffee and maybe just a piece of fruit until night time, and in the evening eating around 1200 calories. I have lost 10 pounds and I feel better. if we listen to our hunger, we only need to eat once or twice a day. Americans eat 3 meals a day and snack all the time, ever wonder why we are such an obese nation?
Hey @jmehta,
in my opinion, it is absolutely necessary for everyone to reflect its own lifestyle.
I will come back to this issue at the end of this series.
Physical activity, food intake and the quality of the food you consume as well as other factors of your lifestyle (sleep, stress, resting time) are major contributors to your health.
The intake of substances such as drugs, medicine and more is just the necessary evil (except for special cases) when you failed to maintain a healthy lifestyle.
To avoid the consumption of snacks & Co. is a good start for a change.
Keep on and post more concerning this and as you dealt with this subject.
Regards
Chapper
Congratulations @chappertron! You have completed the following achievement on the Steem blockchain and have been rewarded with new badge(s) :
Click here to view your Board of Honor
If you no longer want to receive notifications, reply to this comment with the word
STOPDo not miss the last post from @steemitboard:
Hi @chappertron!
Your post was upvoted by Utopian.io in cooperation with @steemstem - supporting knowledge, innovation and technological advancement on the Steem Blockchain.
Contribute to Open Source with utopian.io
Learn how to contribute on our website and join the new open source economy.
Want to chat? Join the Utopian Community on Discord https://discord.gg/h52nFrV
Haha, funny stuff!
Cheers