Hello everyone... In this opportunity I would like to develop the topic of medical management of open wounds on the chest, which are an emergency situation and put at risk the life of the patient.
This type of situation is typical of the trauma-shock area, but every general practitioner should know the basics regarding the initial management of the patient and then be assessed by sub-specialties, such as surgery.
The open thoracic wounds can have different shapes and sizes, being able to share an open communication between the external environment and the pleural space, however being the most common thing that these injuries are sealed by the soft tissues of the chest wall.

Public domain image Photo by: Airman Joseph Thompson
History
The thoracic wounds date back to 3000 B.C., where the first document called The Papyrus, by Edwin Smith, narrates the case of 58 patients, of which only 3 cases are wounds in the thorax itself, the treatment consisted of covering the wound with fresh meat on the first day and the following days with honey, fat and lint.
During the classical era, chest wounds were fatal. Galen treated his army of gladiators with poultice and left the wound open. Thus he lost for many years and it was not until the time of Theodoric in 1267, who recommended the closure of thoracic wounds, and describes that the closure of the wound should be with stitches in the shape and direction of the wound, preserving the natural color of the skin and not allowing air into the chest cavity.
However, not everyone in the medical area followed his advice, as in the case of the military surgeon Paré, who kept the wounds open for 2 to 3 days to allow the blood to drain and then closed it. William Hewson, in 1767, observed that a patient with a large, open chest wound improved his breathing pattern by immediately closing the wound and decreasing complications.By the end of the First World War the controversy of closing or not closing the wound had been resolved in favor of closing the wound immediately, the physiopathology of negative intrathoracic pressure was established that played in favor of wound closure.
By 1875, internist Buelau introduced the closed water seal drainage of an empyema. After several studies and proposed techniques death by thoracic injury, decreases steadily with each war, for example in the Crimean War 79%, Franco-Prussian War 55.7% World War I 24.6% and World War II 12%.
Positive pressure ventilation was practiced in the early 90's, being one of the great medical advances.
Physiopathology
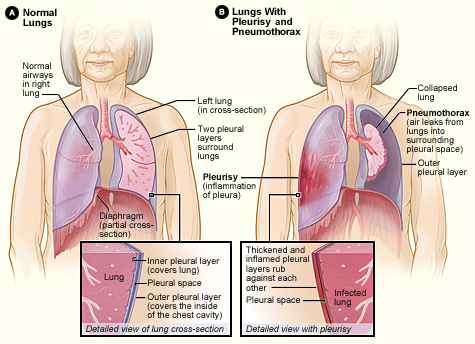
The pathophysiology of open pneumothorax has not changed much since the days of Hewson and Larrey. The pathophysiological changes of blowing thoracic wounds depend on the size of the wound, the integrity of the pleural space and the lung.
In large lesions involving the chest wall and cavity, it causes air movement to move the lung inwards homolaterally and collapse it during inspiration.
The mediastinum may also be compromised by exerting a kind of sway, moving towards the healthy lung during inspiration and towards the injured lung during exhalation, compromising the function of the healthy lung and the injured lung.
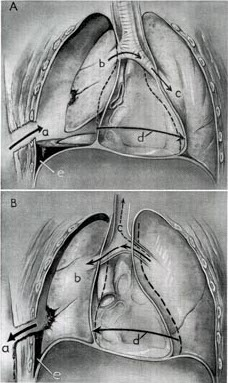
This compensatory mechanism results from a functional dead space between the healthy lung and the injured lung, associated with the progressive loss of ventilation of the diseased lung, which generates asphyxia, hypoxia and hypercapnia.
We must bear in mind that a patient with an open pneumothorax can present in several forms, either asymptomatic and stable or a patient with dyspnea, agony and progressive desaturation in severe cases. And this is proportionally relative to the size of the chest wall lesion, lung lesion, and adjacent structures.
Anatomy
The human body is a complex and diversified system. The thorax is no exception, we can define it as a box-shaped structure containing multiple vital organs.
It is composed of osteocartilaginous structures among which we have, vertebral bodies, ribs, sternum, and multiple joints such as, costovertebral, costotransversa, Inter chondrales, sternal manubrium, and xifoesternal, as well as ligaments and muscles proper to the chest wall.
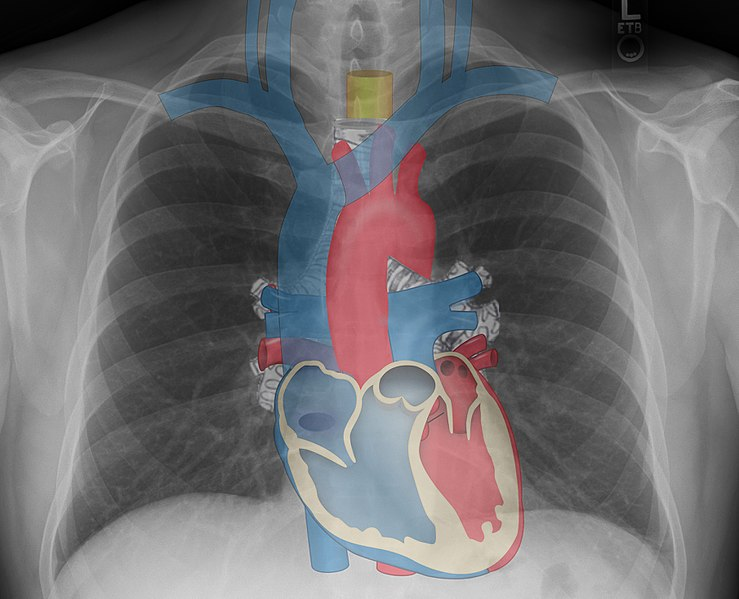
It is well delimited between the trachea in the upper part and the diaphragm in the lower part, including or sheltering the heart, lungs, mediastinum, vascular structures such as the aorta with its ascending, arch and descending portion, the inferior vena cava, ganglion chains among others. It is for this reason that it is called the rib cage.
Indications
The diagnosis of these lesions can easily be made in the event of the evident presence of a chest wall defect, taking into account the characteristics of noise resulting from air movement during inspiration and expiration.
Any patient with respiratory symptoms and open chest wound should be treated immediately. To date, the use of occlusive dressings on the wound is maintained and recommended, leaving a small uncovered portion, that is, if the wound is occluded in its entirety, an open pneumothorax can become a tension pneumothorax.
Now we must clarify, if we have the same patient but in a hospital ward, the wound must be completely closed and immediately place a chest tube.
Radiographic controls are essential in these cases, especially the asymptomatic patient with an open chest wound, in order to determine the integrity of the structures located in the rib cage.
Contra-indication
There is no absolute contraindication for placing occlusive dressings on three sides of the wound leaving a small exit. Until its resolution in a trained hospital area.
These dressings should be placed in an appropriate manner avoiding progression to a tension pneumothorax, which is what happens when the wound is closed completely without the placement of a chest tube.
Materials required for the procedure
Patient Preparation
The patient's time and preparation will depend on the patient's breathing pattern, hemodynamic and ventilatory commitment. In general, informed consent is not required, since the clinic with which he is attending establishes him as an acute patient that must be resolved as soon as possible. And that such a procedure is not invasive and would save the patient's life.
The procedures to be described should be performed quickly, ideally in these cases would be to connect the patient to a heart monitor, pulse oximeter and supplement with oxygen by facial mask, until its full resolution with thoracic tube collation, or surgical procedure based on their condition.
If the patient has severe respiratory failure, orotracheal intubation should be performed before or simultaneously with the application of occlusive dressings in the open wound or closure with sutures and resolution of the pneumothorax with thoracic tube placement according to the medical management and which would be the final result and that this procedure was explained and developed in articles prior to the current one.
Positive pressure ventilation through the endotracheal tube will expand the collapsed lung and force intrapleural air out of the wound.
In those cases where the patient is asymptomatic or slightly asymptomatic, we can take a little more time and prepare the patient, especially in the chest area that is affected, as we could clean the wound, based on asepsis and antisepsis measures and finally place the occlusive dressings on the 3 sides as described below.
Remember and be clear that if the patient moderate to severely symptomatic respiratory does not require preparation, since time is valuable and can cost life, we proceed to occlude the wound with 3 dressings at each end, so that this is resolved later either by the surgery service, pneumology or emergentology.
Technique
The initial and safe treatment of a symptomatic blowing wound is the careful placement of a dressing with vaseline impregnated gauze covering only 3 corners or sides of the wound, preserving a small unoccluded portion.
The dressing should extend 6 to 8 cm beyond the wound margins so that it is not aspirated into the pleural cavity in spontaneously breathing patients.
Cover the vaseline gauze with dry 4 x 4 gases.
Finally apply benzoin tincture around the 3 sides of the dressing and fix it with adhesive to secure the occlusive cap.
An alternative to vaseline dressings is full closure with suture as long as a chest tube can be placed quickly. This method is mostly used in a hospital and non-hospital area such as the use of dressings.
After-care
What continues, in relation to these patients, is the immediate performance of thoracotomy with a tube, with total closure of the wound, cleaning of the wound and covering with intravenous antibiotics for at least 72 hours, to avoid complications of infectious origin both from the wound and from the presence of the tube.
Continuous monitoring of both cardiac and respiratory patterns is essential. They are indicators of the patient's satisfactory clinical evolution.
Pain is a frequent topic of these patients and should be treated with parenteral analgesic drugs or in extreme cases with regional analgesic or intercostal blocks.
Open chest wounds are easily diagnosed by both the evident defect in the chest wall and by the auscultation of the evident air coming out of the pleural cavity.
This type of injury should be treated as soon as possible because it represents a true life-threatening emergency. If the patient is in an outpatient area, an outpatient network, since the application of a dressing on 3 sides is an option and thus stabilize the patient and refer to a complex unit with medical specialties.

Public domain By Ilka Cole, Team Eglin Public Affairs / Published February 08, 2016
Always avoid complications such as tension pneumothorax, when completely obstructed by the dressing, or infectious processes secondary to asepsis and inadequate antisepsis. Once the patient is stable with his chest tube, the wound is thoroughly cleaned and closed with sutures, the use of parenteral antibiotics is essential.
Sources:

steemSTEM is a project of the chain of blocks that supports the scientific content in different areas of science. If you want to know more about this wonderful project you can join the server in discord
This article will be published at https://www.steemstem.io/
link
I hope you enjoyed my content.
Hello,
Your post has been manually curated by a @stem.curate curator.
We are dedicated to supporting great content, like yours on the STEMGeeks tribe.
If you like what we are doing, please show your support as well by following our Steem Auto curation trail.
Please join us on discord.
Thank you very much
This post has been voted on by the SteemSTEM curation team and voting trail. It is elligible for support from @curie and @minnowbooster.
If you appreciate the work we are doing, then consider supporting our witness @stem.witness. Additional witness support to the curie witness would be appreciated as well.
For additional information please join us on the SteemSTEM discord and to get to know the rest of the community!
Thanks for having used the steemstem.io app and included @steemstem in the list of beneficiaries of this post. This granted you a stronger support from SteemSTEM.
Very grateful for the support during my stay at steem. Thank you :)
Congratulations @anaestrada12!
Your post was mentioned in the Steem Hit Parade in the following category:
Thank you for support @arcange
You're welcome @anaestrada12
BTW, feel free to support back and vote for me as a witness