This topic presents one of the essential and important basic aspects in emergency medicine, vital in many situations, which allows us to preserve life if handled correctly, through what is called airway support.
The control and preservation of the airway is crucial, without oxygen, the brain is the main affected and therefore dies in a matter of seconds. The main objective of any emergency physician in these cases, especially a polytrauma patient, is to facilitate the transport of oxygen to the lungs, avoiding contamination of the airway with blood, food and other fluids, which can obstruct the airway, or even trigger acute complications such as bronchial aspiration.
There are times when the management of the airway is so simple that simply elevating the jaw in an unconscious patient with snoring improves the breathing pattern and percentage of saturation, as well as other situations where the idea to preserve the airway will only be through intubation with a fibrobronchoscopy.

Public domain Pxfuel
In these cases time is always critical and short, since an individual can become saturated in a matter of seconds, secondary to injury, obstruction, trauma to the airway and after less than 5 minutes of apnea the patient may have irreversible brain damage.
We must always take into account when treating an unconscious patient, to ensure their airway and their own ventilation capacity, since despite having a spontaneous ventilation, they have a high risk of bronchial aspiration of gastric content, and obstruction of the airway, which puts their lives at risk.
In relation to the patient who is conscious, but with an altered respiratory pattern, we must inspect and check the airway, since such respiratory failure may be the result of obstruction by a foreign body, laryngeal edema, over-infected neoplastic processes, among others.
Anatomy of the via area and physiopathological alterations
This small portion of the human body called the airway comprises the nasal and oral cavity, the larynx, the pharynx and the trachea. Physiologically, these structures are responsible for heating and filtering the air that enters and reaches the lungs and simultaneously allows the passage of food into the digestive tract without complications.
This sophisticated system then allows us to perform essential functions such as eating, breathing and speaking simultaneously, without any difficulty.
The first portion comprises the nasal cavity and the nasopharynx, which corresponds to the area from the tip of the nose to the palate. This area is richly irrigated by thousands of capillaries and blood vessels and innervated by branches of the ophthalmic and maxillary trigeminal nerve.
At the level of the oropharynx, the first structure observed is the tongue and its base, it is innervated in its anterior two thirds by the lingual nerve branch of the facial nerve, while its posterior portion, the tonsils and the palate are innervated by the glossopharyngeal nerve. It is important to take into account the location of the salivary glands and their main function which is to produce a significant volume of saliva and cause problems when ventilating and intubating a patient.
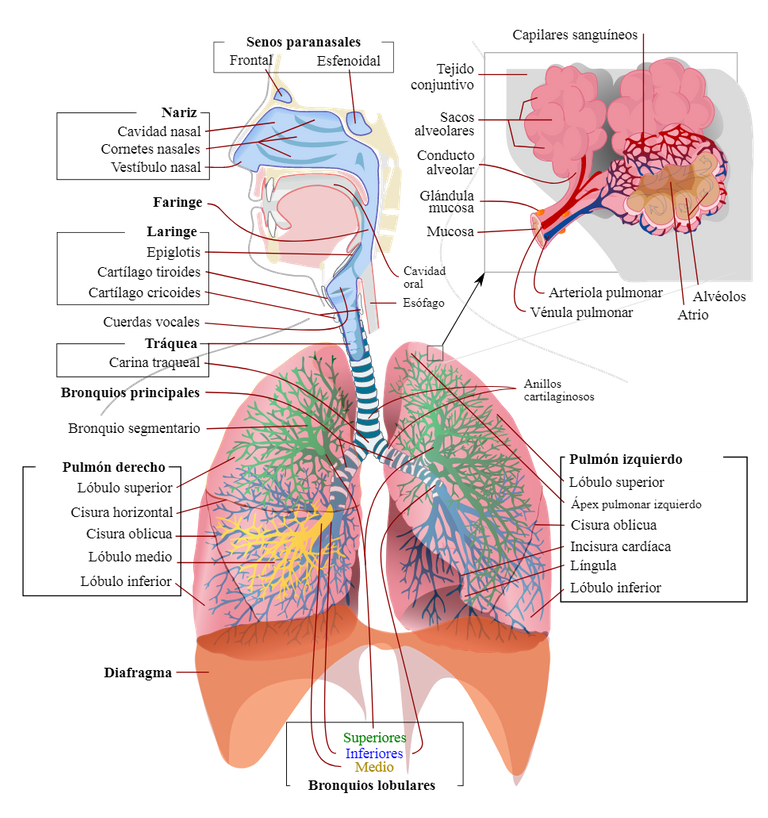
Human respiratory system. Public domain Wikipedia
Also, the presence of loose teeth which should be identified and extracted as a safety measure since they can reach and obstruct the airway, or failing that, the absence of teeth represents a problem when ventilating the patient since there is a loss of structure and anatomy.
The larynx has the capacity to act as a sphincter, made up of 9 cartilages: 3 odd and 3 even.
Odd: epiglottis, thyroid cartilage and cricoid.
Pairs: arytenoid, corniculate and cuneiform cartilage.
Sensory and motor innervation of the larynx is determined by the vagus nerve and its branches.
Finally, the trachea, a structure composed of 17 to 18 cartilaginous rings, in the shape of "C", with an approximate length of 15 cm in the adult.
Indications
The decision to initiate airway support is purely clinical and will be determined by the patient's signs and symptoms in relation to the involvement of the breathing pattern, ventilation and oxygenation.
These clinical signs are usually:
The final signs that indicate the need for respiratory assistance are hypoxia and hypercapnia.
The most frequent etiologies are usually traumatic, intoxication by illicit substances, infectious and cardiovascular processes, obstructive due to the presence of foreign bodies, among others.
Techniques
Patient's position
Airway management and support will depend on the patient's ability to breathe spontaneously or not and whether the airway is permeable.
One of the most important steps when examining the patient is to check that the patient is in the correct position, and that the success of the airway management depends on this.
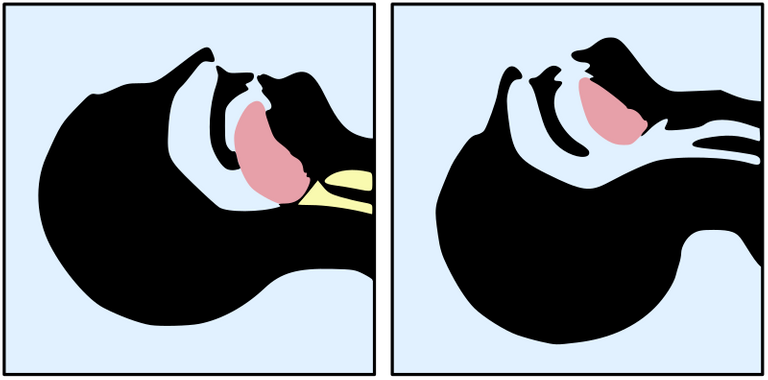
If we suspect respiratory dysfunction is the result of a foreign body, it is recommended that the patient be placed in the Snort position or lateral decubitus, which consists of flexing the cervical spine to about 15 degrees and extending the atlanto-occipitaly joint to the maximum. A position that we usually adapt in a common way when trying to smell, smell flowers aromas.
This position is achieved by raising the chin. Those patients who are obese and have large breasts, it is advisable to place the patient in an elevated position, leaning with a roll of cloth under the shoulders to achieve the snorting position.
Jaw thrust
It is one of the most basic and used, is based on pulling the jaw with two hands while, with the help of another person, provides positive ventilation. The idea is to take the angles of the jaw and move it forward.
Public domain CC BY-SA 3.0
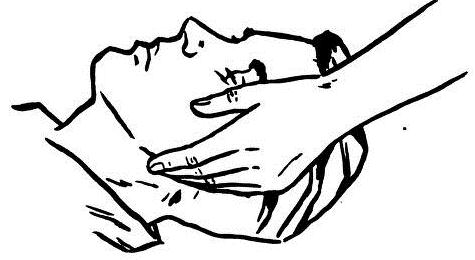
Chin Lift Maneuver
Similar to the one already described, very simple and basic to secure airway, and consists of raising the jaw in the anterior and cephalic direction, placing the fingers under the jaw. The head must be inclined in a posterior direction and in this way clear and open the airway.

Public domain CC BY-SA 3.0
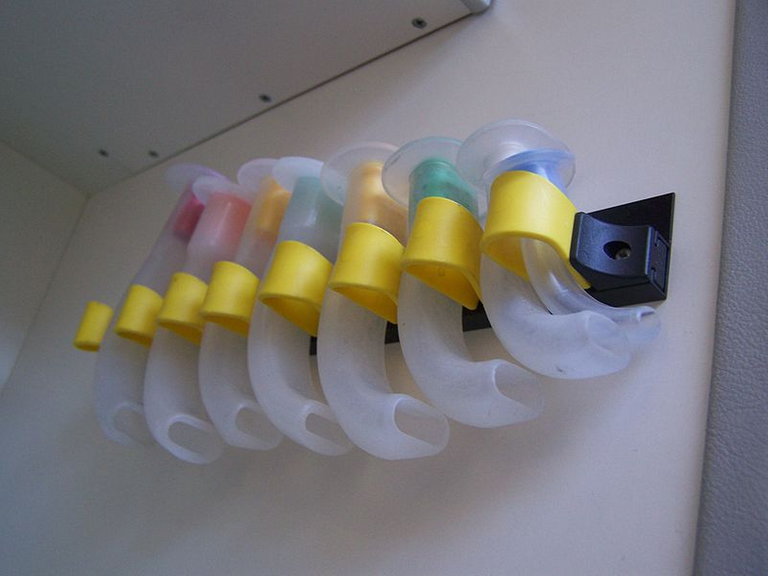
Nasopharyngeal Cannulas
We must take into account that most obstructions occur at the level of the pharynx and that a correct position of the patient helps us to overcome the site of obstruction and achieve ventilation and for this we use the so-called Nasopharyngeal and Oropharyngeal Cannulas.
Nasopharyngeal cannulas are made of soft rubber or plastic material and come in various sizes, can be used safely in unconscious patients. Conscious or semi-conscious. It is used when the use of the oropharyngeal cannula is contraindicated (in cases of oral trauma).
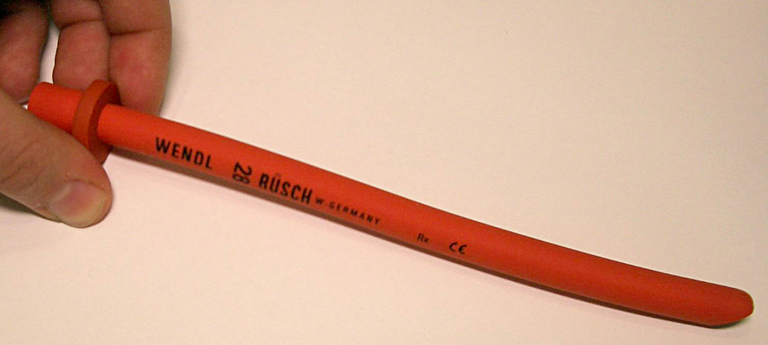
To use this device it is mandatory to perform a jaw thrust or chin lift to prevent the tongue from obstructing the airway.
Before placing the cannula, it is advisable to apply abundant water-soluble lubrication or analgesic gel, proceed to carefully insert the tube with its beveled part towards the nasal septum, insert it up to the flared end and rotate it about 90º, as it is concave upwards.
If resistance is encountered during insertion, it should be rotated a little, and it is recommended that oxygen be placed through the mask during the procedure.
The most frequent complications are: laryngospasm, vomiting, gastric distension with high risk of aspiration, epistaxis.
Oropharyngeal Cannula
This procedure is simpler and with less risk of complications. Its function is to keep the airway clear and to move the tongue away from the back wall of the pharynx. It should only be used in unconscious patients, since if placed in active and vigilant patients it triggers laryngospasm and vomiting as an adverse effect.
We take the correct size, 8 to 9 cm in most adults. We proceed to open the mouth with a scissors maneuver, placing the thumb on the lower teeth and the middle and index fingers on the upper ones, once the oral cavity is visualized, the cannula is inserted downwards and rotated at about 180º so that the curve follows the tongue.
If the procedure is not performed correctly, we can push the tongue back and obstruct the airway, lacerate the tongue or lips, and even move the epiglottis against the vocal cords and obstruct the airway.
This cannula has several functions, the most important being to keep the airway permeable, but it is also useful to prevent the patient from biting, lacerating or occluding the endotracheal tube, and it facilitates aspiration.
Mask Ventilation
The determination of whether to use a mask or intubation will depend on the patient's clinic, his anatomy and the structural alteration of the mask.
Ideally, the patient should be held in the correct position as described above, to evaluate the breathing pattern and determine whether or not breathing is spontaneous.

If the patient is not breathing and there is no evidence of a foreign body, ventilation should be initiated with positive pressure.
Once the area is clear, proceed to induce positive pressure ventilation, either by mouth-to-mouth, mouth-mask or mask ventilation.
The key to effective mask ventilation is to ensure a patent airway in combination with certain maneuvers such as jaw thrust and chin lift with the patient in the snorting position.
The face masks are made of plastic and/or silicone material, with a cushioned seal and an anatomical shape to fit the contours of the face. The ideal adult size is 3, 4 and 5. Ideally, the mask should be large enough to cover the mouth and nose, but not so large as to allow leakage during ventilation.
There are two ways to fit the mask correctly.
The technique with one hand, in this case the left hand, where the ring and middle finger are placed on the left side of the jaw, while the thumb and index finger are placed on the lower and upper part of the mask and finally the right hand is used to lift the jaw and extend the atlanto-occipital joint simultaneously, allowing the passage of positive pressure.
The two-hand technique is useful in elderly, obese, bearded or edematous patients, where both hands are placed over the mask to avoid leaks and to align the airway, after the patient has been placed in the snorting position. If the patient is not ventilated after adequate positioning, various manoeuvres already described, a cannula is placed as indicated after assessment and if ventilation is still difficult and the patient's life is compromised, tracheal intubation should be started immediately.
Complications
Among the complications we have the bronchoaspiration of gastric content, blood, food and other fluids, which triggers devastating infectious processes.
While soft tissue injuries such as lip laceration, tongue, oral cavity, epistaxis are usually less severe and resolve if more important.
Conclusion
In general, the basic handling of an area is vital in every emergency physician, and that, above all, that doctor on duty must have the material at hand, to have an effective response in these emergency cases, such as masks, cannulas, gloves and even tweezers to remove foreign bodies, and never rule out the possibility that at some point the patient may need an intubation, for which they must always be prepared.
Sources:

steemSTEM is a project of the chain of blocks that supports the scientific content in different areas of science. If you want to know more about this wonderful project you can join the server in discord
This article will be published at https://www.steemstem.io/
link
If you have any questions about any topic of medicine or present any disease you can comment the publication or write me in discord and I will attend you.
Dr. Ana EstradaI hope you enjoyed my content.
@anaestrada12, thank you for supporting @steemitboard as a witness.
Click on the badge to view your Board of Honor.
Once again, thanks for your support!
Do not miss the last post from @steemitboard:
Excellent technique. Dra thanks for sharing this information.
This post has been voted on by the SteemSTEM curation team
and voting trail. It is elligible for support from @curie and @minnowbooster.
If you appreciate the work we are doing, then consider supporting our witness @stem.witness. Additional witness support to the curie witness would be appreciated as well.
For additional information please join us on the SteemSTEM discord and to get to know the rest of the community!
Thanks for having used the steemstem.io app and included @steemstem in the list of beneficiaries of this post. This granted you a stronger support from SteemSTEM.