THE SCIENCE OF THE HUMAN EYE AND ITS EXAMINATION – STEREOPSIS
The Eye is an organ (a collection of tissues performing the same function) in the human system which function is for vision. Vision has to do with the ability to perceive things.
The eyes pick up light signal from the surrounding and convert it into impulses in the neurons. The neuron is a cell of the nervous system which conducts nerve impulses. The nervous system is the system that is responsible for coordinating the activities of muscles, monitor organs, constructs and processes data received from the senses and initiates actions.
An image is formed when it focuses the light on the lenses; the image is converted to electric signals which are transmitted to the brain through complex neural pathways that connects the eye through the optic nerve to the visual cortex and other parts of the brain.
THE PARTS OF THE HUMAN EYE
THE SCLERA
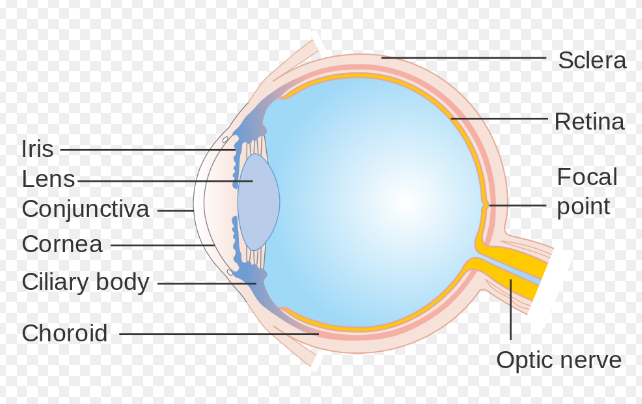
Image from Wikimedia
The Sclera is the thick connective tissue of the eyeball that forms the “White” of the eye. It is continuous with the stroma layer of the cornea. The junction between the White sclera and the clear cornea is called the limbus.
The exterior of the sclera is smooth and white while the interior is brown and grooved; it has tendons attached to it. The grooves in the sclera helps the tendons of the eye attach properly. It provides structure and safety for the inner workings of the eye, it is extremely durable and flexible and strong, this is due to the interwoven arrangement of the fibrils of collagen.
Metabolically the sclera is relatively inactive and has a limited blood supply. Blood vessels pass through the sclera to other tissues, but the sclera is considered avascular.
THE CORNEA
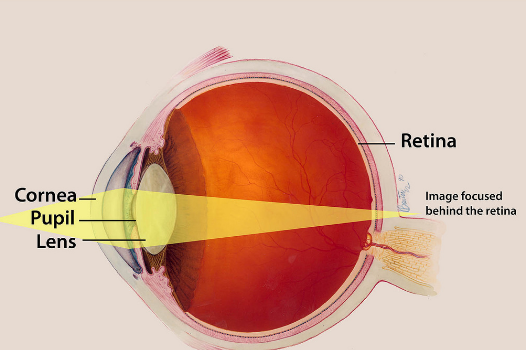
Image from Flickr
This is the outer covering of the eye, it is dome shaped and protects the eye from hazardous elements.
The cornea is the major refractive surface of the eye. It consists of three main layers. These layers regenerate very quickly, aiding the eye to cure damages more efficiently. The cornea also helps the eye to focus on light effectively.
The stroma is the densest layer of the cornea which lies behind the epithelium. It consist mostly of proteins and water which gives it an elastic but solid form.
The endothelium is located behind the stroma. It is a single layer of cells. It is in constant contact with the aqueous humor.
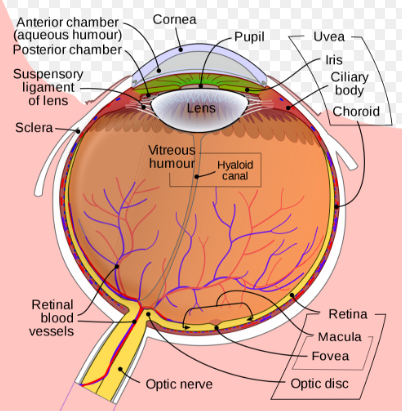
Image from Wikipedia
The stroma absorbs excess liquid and the endothelium pulls it out. Without this function, the stroma would become waterlogged and as a result the cornea would get opaque and hazy and results in blurred vision and may result in increase fluid pressure in the eye (Glaucoma).
The epithelium is the outermost layer. It prevents outside objects from entering the eye.
THE IRIS/PUPIL
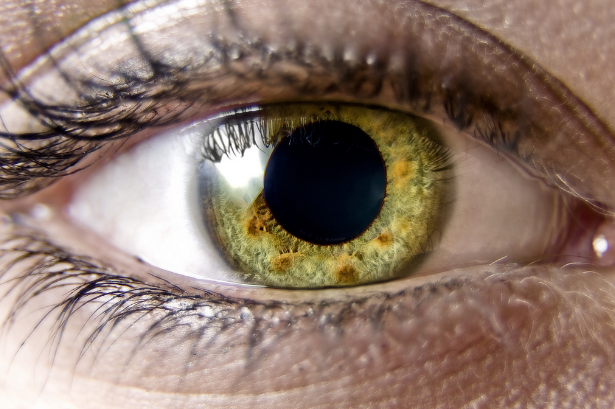
Image from Pixnio

The pupil appears as a black small circle in the middle of the eye between the cornea and the lens that is perforated by the pupil. It is covered by a transparent fluid known as the aqueous humour. The diameter of the iris is 12mm and it regulates the amount of light that enters the eye with the aid of two sheets of smooth muscles with contrary actions; dilation (expansion) by the dilator muscle and contraction (constriction) by the spincter muscle.
The colour of the iris is determined by the amount of pigment contained in it. The iris appears blue when the pigment is very little, when the pigment contained it increases the colour shade become deep brown to black.
LENS
Image from Timesofisrael
The lens is a biconvex structure behind the iris, with sole function of focusing light rays towards the retina. It is made up or elongated avascular cells with the aqueous humour which cleanses the lens and removes waste products. In order to focus clearly on objects the lens is altered by expansion and constriction thus changing the shape of the lens. The lens can adjust from a distant to near focus this phenomenon is called Accommodation.
RETINA
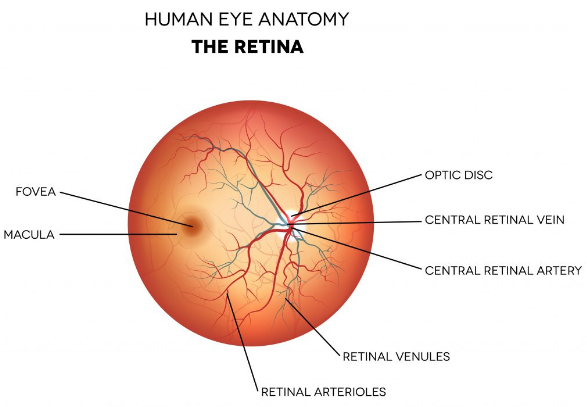
Image from Consultingeye
The retina consists of a layer of nervous tissues which cover the inside of the back two-thirds of the eyeball known as the Macula, in which stimulation by light occurs, initiating the sensation of vision.
It is made up of rods and cones arranged in layers which will transmit light into chemicals and electrical pulses. The macula helps to interpret the details of the object is seeing with the aid of the fova (center of the macula) which increases the detail of the images to a perceivable point.
The retina is actually an extension of the brain formed embryonically from neural tissue and connected to the brain.
Image from Wikimedia

VISUAL ACUITY
Visual acuity can simply be defined as the clarity of vision. It is a measure of the spatial resolution of the visual processing system or the visual performance.
It depends on certain factors like the functioning of the retina and its sharpness focus with the eye as well as the sensitivity of the brain. Low visual acuity could be caused by refractive error or other eye defects. With respect to the length of the eyeball, too high or too low refractive error is the culprit of myopia (shortsightedness) of hypermetropia (longsightedness). Another anomaly is astigmatism. Most of these defects could be corrected by optical lenses like eyeglasses, contact lenses etc.
THE DEFECTS OF THE EYES AND THEIR CORRECTIONS
MYOPIA
Image from Wikimedia

Myopia which is also known as shortsightedness or nearsightedness is a defect of the eye where light focuses in front of instead of on the retina. With this, distant objects become blur, a s such victim will be unable to see far objects clearly while near objects appear normal. Headache and strain could be observable symptoms, while genetic and environmental factors could be the cause.
Myopia could be corrected with eyeglasses, surgery or contact lenses with the first being the easiest and safest, the second providing wider field of vision and the third having a risk characteristic respectively.
A concave lens is used, it’s depressed into the lens and helps to bring the image light from “infront of” to settle “on” the retina.
HYPEROPIA
Hyperopia and myopia are both defects of the eyes with the former being called farsightedness (in ability to see near objects clearly) while the former is nearsightedness (inability to see far objects clearly). Like myopia, headaches and eye strain are associated symptoms.
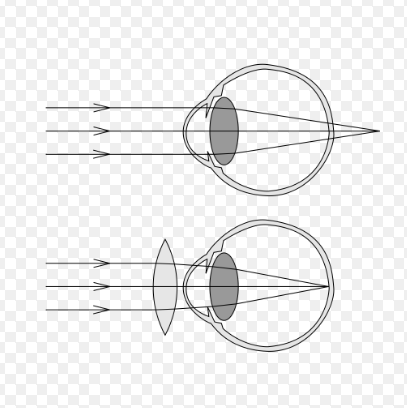
Image from Bateseyeexercises
In Hyperopia, light is focused behind instead of on the retina making near objects appear blurry.
It could be corrected through eyeglasses, contact lenses and surgery too. Abnormal shape of the retina and low converging power of the eye lens are the main causes. Convex lenses are used to remedy the issue. A convex lense bulges outward from the lens which brings the light from behind to appear on the retina for normality.
ASTIGMATISM
Image from Wikimedia
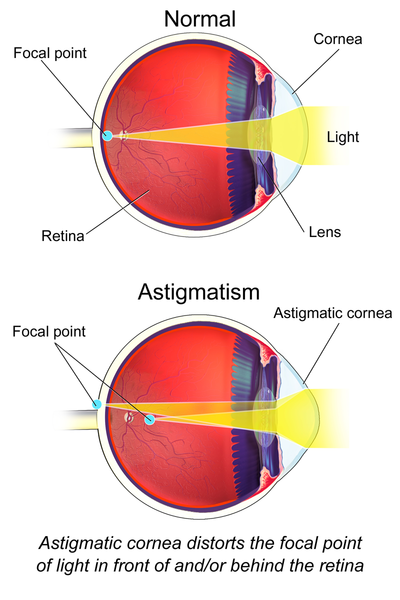
This is another refractive error which describes the inability of the eye to focus light evenly on the retina. It results in blurred vision and then headache as a symptom. The cause is not really certain, but accepted to be genetic. It is diagnosed by eye exam and could be treated with the same means.
Following DR. Bazuaye's triad method of clinical procedure in Eye Examination - STEREOPSIS
ACCEPTABLE DEFINITION
1. OPERATIONAL DEFINITION OF TERMS AND CONCEPTS
Stereopsis is a term that is most often used to refer to the perception of depth and 3-dimensional structure, obtained on the basis of visual information derived from the two eyes from individuals with normally developed binocular vision system.
Image from Wikimedia

HISTORY/BACKGROUND INFORMATION
Stereopsis was first explained by Charles Wheatstone in 1838. The mind perceives an object of three dimensions by means of two dissimilar pictures projected by it on the two retinae surfaces.
Leonardo Da Vinci had also realized that objects at different distances from the eyes project images in the two eyes that differ in their horizontal position.
The Howald-Dolman(HD) two-rod apparatus is the gold standard for measuring stereo acuity (steropsis), amongst others. Visual acuity is a measure of how we see small objects.
2. PRINCIPLES OF OPERATION AND DEVELOPMENT/CONTRIBUTORS
In stereopsis test (stereotests), slightly different images are shown to each eye, such that a 3D image is perceived if stereovision is prevented. This can be achieved by means of vectographs, analygraphs, lenticular lenses or hand-mounted dispalay technology.
3. USAGE AND CARE/MAINTENANCE
Strereopsis test is used to ascertain perfect working conditions of the binocular retinal disparity function of an individual's eyes.
Image from Wikimedia

CLINICAL RELEVANCE
1. INDICATIONS
To test for binocular retinal disparity functions
Contradications:
For people with binocular retinal disparity problems.
Limitations:
Laboratory measurements are affected by refractive blurry and strabusmus.
2. ADVANTAGES, DISADVANTAGES AND SIGNIFICANCE
ADVANTAGES
It can easily be performed using a stereoscope and it is popularly recognized.
DISADVANTAGES
It is associated with hysteresis effect and it is different for both eyes.
SIGNIFICANCE
It's used for testing proper binocular retinal disparity function.
3. PRECAUTIONS, INTERPRETATIONS AND ALTERNATIVE PROCEDURE
PRECAUTIONS
- The target must be held at exactly 40cm in front of the eyes
- Proper illumination must be observed.
- The patient's sitting position must not be altered.
INTERPRETATION
Stereopsis gives a practical approach towards determining a patient's fine depth perception through his ability to fuse stereoscopic targets.
ALTERNATE PROCEDURE
This can be done using the American optical vectogaraph slide, while the patient wears a Polaroid glass.
CLINICAL ASPECT OF STEREOPSIS
STAGE 1
W1: ASSEMBLING STAGE FOR INSTRUMENTS.
STEP 1:
- Main instruments: polaroid glasses or red-green glasses depending on the test used.
- Stereo test booklet (eg. Randot, Titmus, Bernell, TNO test).
Alternative instrument: American optical vectographic slide.
SOLIDS: Polaroid glasses, stereo-test booklet, red-green glasses, American optical vectographic slide, and overhead lamp.
Image from Wikimedia

W2: BUILDING UP OF TEST INSTRUMENT AND PATIENT (OR MEASURING INSTRUMENT AND LENS)
STEP1: BUILD UP THE TEST OR MEASURING INSTRUMENT BY MEANS OF:
Standardizing through focusing of eye piece, selection of weights etc.
The target is a state target and should be held at 40cm in front of the patient with an overhead lamp directed towards the target.
The Polaroid glass or red-green glasses will be worn by the patient over his bear correction point.
Sterilizing with cotton wool, alcohol, etc.
The Polaroid glasses and the red-green glasses will be cleaned/sterilized with alcohol using cotton wool.
Setting up the instruments by coupling, selecting and positioning of the instruments.
The Polaroid glasses/red-green glasses will be mounted on a lens frame and the stereo target will be positioned 40cm parallel in front of the patient's eyes.
STEP 2: BUILD UP THE PATIENT OR OPHTHALMIC LENS/CONTACT LENS.
Image from Flickr
VERBALLY:
What (I want to see how your two eyes work together),
Why (to measure your fine depth of perception)
Which (is a measure of your ability to fuse stereoscopic targets).
VENTAGE POSITION AND POSTURE ASSUMED:
Positions (patients should sit upright and look through the Polaroid glasses or red-green glasses, no head tilt),
Angles (90• between thigh and trunk, head should be parallel to trunk on both sides),
Distances (patients should sit at 40cm from the stereo target).
VISUALLY:
Accessories (a Polaroid glass or red-green glass is worn by the patient on the face),
Laterally (binocular),
Lighting (target object should be adequately illuminated and room light should be adequate).
W3: COMMENCEMENT OF COORDINATED MEASUREMENT OR EXAMINATION OR TEST STAGE
STEP 1: Alignment (with or without supports, adjustments or otherwise)
Clinician hands and body posture (position, angle bad distances), should be aligned to the target objects and to the patient's body respectively.
Patient's selected eye (usually the right eye) or eyes should be aligned to the fixation target with specified shape and size of a specified distance (specified earlier on to patient in stage
- The patient is asked to look at the fixation target and ensure it is seen.
Clinician's eye(s) should be aligned to OR through the target objects to the patient's eyes for measurements with rule.
STEP 2: Begin the MET (Measurements or Examination or testing) slowly and steadily
The patient's attention is directed to the smallest set of targets: a set of three or four circles.
The patient is asked to tell what he sees, if the patient is unresponsive, he is asked to identify which of the circles in set number one appeared closest or seem to be floating above the page.
If the patient appreciates stereopsis on the first set of targets, he is instructed to go on to the next set.
The testing would continue until the patient gives two consecutive incorrect answers.
If the patient was unable to correctly identify the floating object in the smallest set of targets, step1 and 2 would be repeated using medium-sized targets. The patient is asked again to identify the object that floated above the page. If the patient identified all of these correctly, the smallest sets of targets is tried again.
If the patient was unable to correctly identify any of the medium-sized targets, he is shown the large targets and if he was able to identify all large targets, the others (ie. Medium and large-sized targets), if done without correction, it is recorded as "sc" if with correction, it would be recorded as "cc".
NOTE
i. The amount of stereopsis is recorded in seconds of arc.
ii. If the patient was unable to correctly identify any of the small targets, the amount of stereopsis would be that of the smallest target the patient was able to correctly perceive.
iii. If the patient did not perceive any of the stereo targets,it is recorded as "NO STEREO".
iv. The name of the test should be recorded.
Example: stereo at N SC 40sec, Titmus.
STEP 3: Conclude the measurements or examination or testing (met)
The MET was repeated until the findings were sure, and these were recorded immediately and clearly.
The MET was repeated for both eyes.
Findings were ordered properly for immediate use.
Gif by @hboi

REFERENCES
Cornea Function, Definition & Anatomy, Published 2nd April 2017 in Eyepaincenter blog, Accessed 19th May 2018 from https://www.eyepaincenter.com/cornea-function/
Tissues that make up the eye, Published 6 October 2013 in Prezi blog, Accessed 19th May 2018 from https://prezi.com/esl-r8aoe1qq/tissues-that-make-up-the-eye/
Visual acuity, Published 6th June in Wikivisually Accessed 19th May 2018 from https://wikivisually.com/wiki/Visual_acuity
Iris anatomy, Published 2015 in Sciencedirece , Acessed 19th May 2018 from https://www.sciencedirect.com/topics/medicine-and-dentistry/iris-anatomy
Common cornea problems, Published 9 December 2017 in Webmd, Accessed 19 May 2018 from https://www.webmd.com/eye-health/cornea-conditions-symptoms-treatments#1
Retina (Anatomy), Published 5 April 2018 in Britannica, Accessed 19 May 2018 from https://www.britannica.com/search?query=retina
Parts of the eye and their functions, Published in Robertsonopt inAccessed 19 May 2018 from https://robertsonopt.com/parts-of-the-eye-their-function/
Iris, Published 19 August 2008 in Britannica, Accessed 19 May 2018 from https://www.britannica.com/science/iris-eye
Lens, Published 22 May 2015 in Britannica, Accessed 19 May 2018 from https://www.britannica.com/science/lens-eye-structure
I like the analyzation of your work and the content .
Very complete and understandable article, this will help me in my studies. Thanks!
Oh friend i'm agree with the last comment very complete article y helpful information for medicine students, Upvoted! @richi-3
Thanks for coming around