Guys, thanks for reading my first entry of the Cranial Nerves from my previous post. Here is the continuation of the prodigious part of the human brain:
CNVII – Facial Nerve

We shall begin with the one of the commonest nerve that might be affected by a disease, which is the CNVII. The facial nerve has mostly motor innervation and a bit of sensory function too. The motor part innervates the muscles of facial expressions (hence the name, facial), posterior belly of the digastric muscle, stylohyoid and the stapedius muscle (another muscle of the ear). The sensory part innervates the small area of the ear known as the concha and the anterior 2/3 of the tongue. It also supplies many glands of the head and neck: the submandibular, sublingual salivary glands. Nasal, palatine, and pharyngeal mucous glands. Also the lacrimal glands.
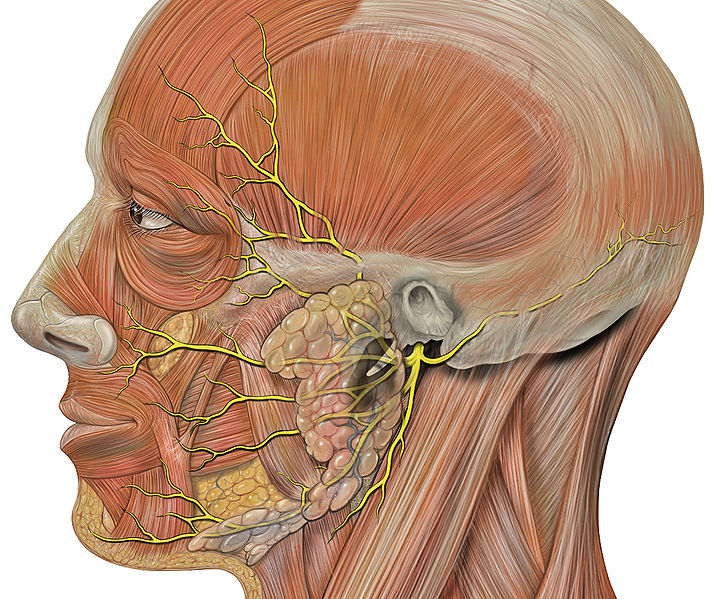
Alright, the anatomical course of facial nerve is quite complex but it’s one of the more important one as compared to the other cranial nerves. This is a common exam question for the undergraduates, so better bear with me. The facial nerve arises from the pons and begins as two roots, the large motor and the small sensory roots. The two roots travel through the internal acoustic meatus and it’s quite close to the inner ear. After leaving the internal acoustic meatus, it enters the facial canal. This canal is a “Z” shaped structure. Interestingly in this canal, two events occured. First, the two separate roots combined into one. Secondly, the nerve give rise to the greater petrosal nerve (supplies the mucous and lacrimal glands) nerve to stapedius (a motor innervation to one of the ear muscle) and chorda tympani (a special sensory fibre to the anterior 2/3 of the tongue). The facial nerve then exits the facial canal via the stylomastoid foramen. Extracranially (which means outside the cranium), the nerve give rise to the posterior auricular nerve (innervation to some muscles of the ear) and motor branches to the posterior belly of digastric muscle as well as the stylohyoid muscles. The remnant main branch of the facial nerve then continues by passing through the parotid gland (you’ll see the clinical importance later) and within this gland, it terminates to form five branches: temporal, zygomatic, buccal, marginal mandibular and cervical branch. These branches are for facial expressions.
Clinical Relevance

The spectrum of illness is quite broad as facial nerve innervates many parts of the head including the face (loss of facial expressions), the ear (hyperacusis), and even the tongue (loss of sensation). Causes of the facial nerve problems can be due to parotid gland pathologies (as I’ve mentioned earlier that the facial nerve terminates at the parotid gland), infection of the nerve, and idiopathic (such as in Bell’s palsy which is quite common).
CNVIII – Vestibulocochlear Nerve
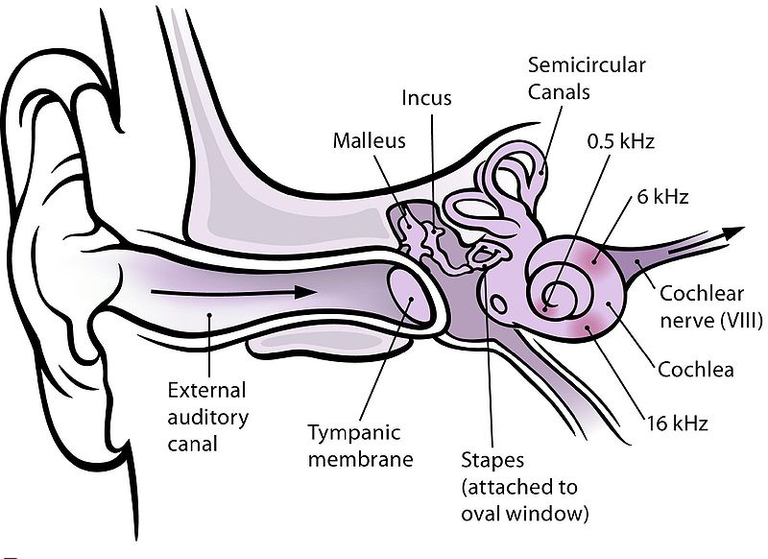
This nerve is purely sensation and it is divided into two components, the Vestibular (balancing) and the Cochlear (hearing) fibres. This nerve emerges from the brain at the cerebellopontine angle (a junction between Pons and Medulla) and exits the cranium via the internal acoustic meatus of the temporal bone. Here, it splits into the Vestibulo and Cochlear nerves.
The cochlear of the ear senses the sound waves and through several processes, the impulse is sent to the cochlear nerve. The vestibular parts of the ear detects the position of head in relation of gravity.
Clinical Relevance
A Basilar skull fracture which is a fracture of the skull base can damage the nerve causing it to produce hearing and balancing symptoms. Vestibular neuritis (inflammation of the vestibular nerve) is another condition that can result in vestibular symptoms such as vertigo, nystagmus, loss of equilibrium and vomiting.
CNIX – Glossopharyngeal Nerve

4 more to go. Alrightt. This nerve has both motor and sensory components. The sensory component supplies the oropharynx, carotid body and sinus, posterior 1/3 of the tongue, middle ear cavity, Eustachian tube and the posterior 1/3 of the tongue. The motor component supplies the stylopharyngeus muscle of the pharynx. This nerve arises from the medulla oblongata and leaves the cranium via the jugular foramen. Here, it gives a nerve to the middle ear for sensation. After that, it descends down to the neck and give motor supply to the stylopharyngeus, sensory branch to the pharyngeal branch (which give rise to the pharyngeal plexus along with the CNX that innervates the oropharynx), tonsillar branch which innervates the palatine tonsils, lingual branch which innervates the posterior 2/3 of the tongue, and a nerve supply to the carotid body/sinus. Interestingly to note that the nerve to the carotid body and sinus provides us information of the blood pressure and oxygen saturation respectively. This nerves also supplies the parotid gland.
Clinical Relevance
It provides sensory supply to the oropharynx, hence it is involved in the gag reflex. Gag reflex happens when a sensation of vomiting is introduced when a foreign body touches the back of the mouth. Absence of this reflex is due to CNIX damage.
CNX – Vagus Nerve
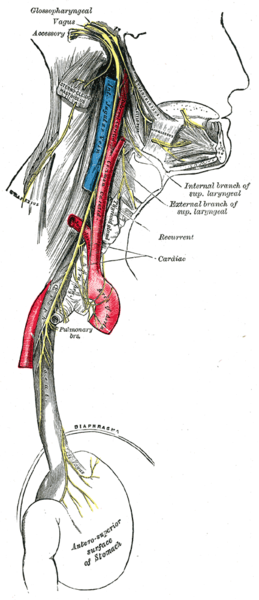
This nerve is a special one as unlike other nerves, this nerve exits the head and even descends as far as our large bowel! The name of this nerve came from the Latin word vagary which means wandering. I’ll describe the anatomical pathway of this nerve and you will understand why this nerve is called as such. Due to the widespread of distribution, Vagus nerve has multiple functions and the clinical cases are pretty much depended on the site of the damage. Interesting to note that the vagus nerve was originally named as the pneumogastric nerve, which probably due to the extensive reach as it goes as distal as the stomach(gastro) region. Due to its various innervation supplies, it’s no surprise that this nerve as both sensory and motor functions.
In the head region, it arises from the medulla and leaves the cranium via the jugular foramen. “Foramen” means passage and this jugular foramen as well provides pathway to two other nerves, glossopharyngeal (CNIX) and accessory (CNXI) nerves. Here, it gives off a sensory branch to the ear, innervating the sensation part of the external auditory and the external ear canal.
Moving southwards in the neck region, it is accompanied by the common carotid artery and internal jugular vein in a covering known as the carotid sheath. At the base of the neck, this nerve splits into the right and left branches. A few branches arise from this neck region including the pharyngeal branch (motor innervation to most muscles of the pharynx and soft palate), superior laryngeal nerve (motor innervation to the cricothyroid muscle of the larynx and sensory innervation to the larynx) and the recurrent laryngeal nerve (innervates most of the laryngeal muscles). In short, it supplies most of the larynx parts.
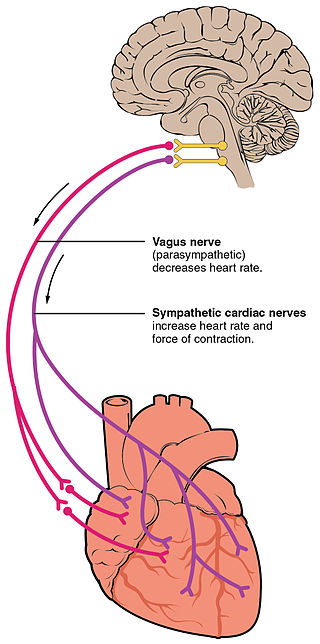
In the thorax region, it innervates the oesophageal smooth muscles, intrinsic muscles of the larynx and even the heart.
How does it helps the heart?
It regulates the heart rate and provide visceral sensation to the heart. Sweet. After that, it moves inferiorly still towards the abdomen by piercing the diaphragm. In the abdominal region, it ends by dividing its branch to supply the remaining part of the oesophagus, stomach, small bowel, and the colon.
In a nutshell, here’s the summary:
Sensory functions
- External ear
- Laryngopharynx
- Larynx
- Heart
- Gastro-intestinal tract
Motor
- Muscles of the pharynx
- Muscles of the larynx
Other functions
- Heart rate regulation
- Gastro-intestinal smooth muscle contractions and glandular secretions
Clinical Relevance
Since it is so widespread in the head, neck, thorax and abdominal region, some diseases like the congenital heart disease such as patent ductus arteriosus can irritate the recurrent laryngeal nerve branch causing the individual to experience hoarseness of voice. Since it innervates the heart, many drugs can be used to influence the heart rate such as Digoxin and Beta-blockers. Apart from that, since it is the efferent pathway of the gag reflex as CNIX controls the afferent pathway, the individual might loss his/her gag reflex.
CNXI – Accessory Nerve
This is an interesting nerve as it comprises of two components, namely the Spinal Part and Cranial Part . This nerve is purely motor as it only innervates muscles.
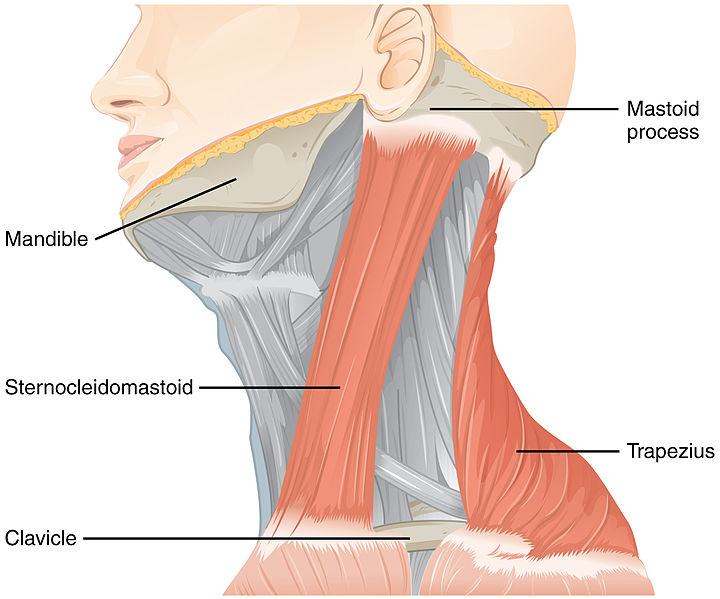
The spinal accessory nerve comes from the columns of upper spinal cord (C1-C5/C6 spinal nerve roots). After exiting the upper spinal cord, it pierces in the skull via the foramen magnum and then it passes through the posterior cranial fossa and it exits again via the jugular foramen. Before it exits, it meets briefly with the cranial accessory nerve. Take note that this is the only nerve that both enters and exits the skull! After exiting the cranium, it travels inferiorly to innervate the sternocleidomastoid muscle of the neck and trapezius. The cranial part is very small and originates from the medulla. It leaves the skull via the jugular foramen where it makes a contact with the spinal accessory nerve. As soon as it leaves the skull, it combines with the Vagus Nerve (CNX). Hence, the cranial part of the accessory nerve is considered to be a part of the CNX.
Clinical Relevance
An interesting fact about this nerve is that the accessory nerve is not that deep in the skin upon exiting the skull. Hence, it has a risk to be damaged in medical procedures such as the cervical lymph nodes biopsy or insertion of line at the internal jugular vein. The individual with damaged CNXI might have partial paralysis of the sternocleidomastoid muscles resulting in the inability to shrug shoulders and to rotate the head.
CNXII – Hypoglossal Nerve
Alright, here comes the final nerve of the cranial nerves, which is the hypoglossal nerve. Hypo means under and glossal means tongue. As the name implies, it innervates the tongue muscle. It is purely motor with no sensory components. This nerve originates from the medulla part of the brain and passes through the posterior cranial fossa and exits the skull via the hypoglossal canal. After exiting the skull, it travels alongside some nerve fibres from the C1/C2 spinal nerve roots. The Hypoglossal nerve travels inferiorly to the angle of mandible, passing through both internal and external carotid arteries and pierces the tongue. This nerve is responsible for all the movements of the tongue.
Clinical Relevance

Problems with this nerve might be caused by tumours or injuries. The individual will experience the deviation of tongue towards the site of damage. Interestingly, the tongue might be twitching (this is called as fasciculations) on the affected site.
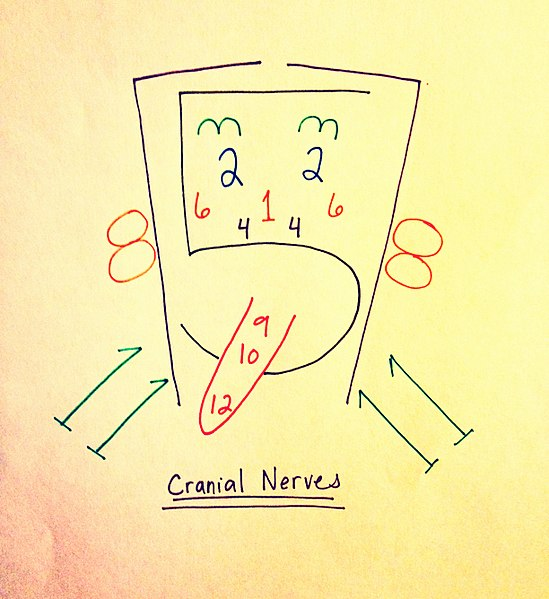
That’s all for today’s entry. In my perspective, the anatomy of the Cranial Nerves is quite difficult to be memorized but by understanding the pathway and the function, we are able to relate it with the clinical features that it provides. Here is a picture for easy memorization of all the 12 cranial nerves! Have a good day everyone :)
References
- The Cranial Nerves. Teach Me Anatomy. Retrieved on April 8, 2018, from http://teachmeanatomy.info/head/cranial-nerves/
- Ultrastructure of Nerves. Teach Me Anatomy. Retrieved on April 8, 2018, from http://teachmeanatomy.info/the-basics/ultrastructure/nerves/
- Cranial Nerve Examination. Geeky Medics. Retrieved on April 8, 2018, from https://geekymedics.com/cranial-nerve-exam/#2
- Cranial Nerves. Wikipedia. Retrieved on April 8, 2018, from https://en.wikipedia.org/wiki/Cranial_nerves
wow nice seeing an interesting post on the nerves at the moment am writing about the median nerve you could check out my blog
checked and commented. Awesome article !
You've been upvoted by TeamMalaysia community. Here are trending posts by other TeamMalaysia authors at http://steemit.com/trending/teammalaysia
To support the growth of TeamMalaysia Follow our upvotes by using steemauto.com and follow trail of @myach
Vote TeamMalaysia witness bitrocker2020 using this link vote for witness