
Hey guys, this is a continuation of my previous blog post. I'll cover the uses of stethoscope in terms of Respiratory and Gastro-Intestinal systems.
Respiratory System
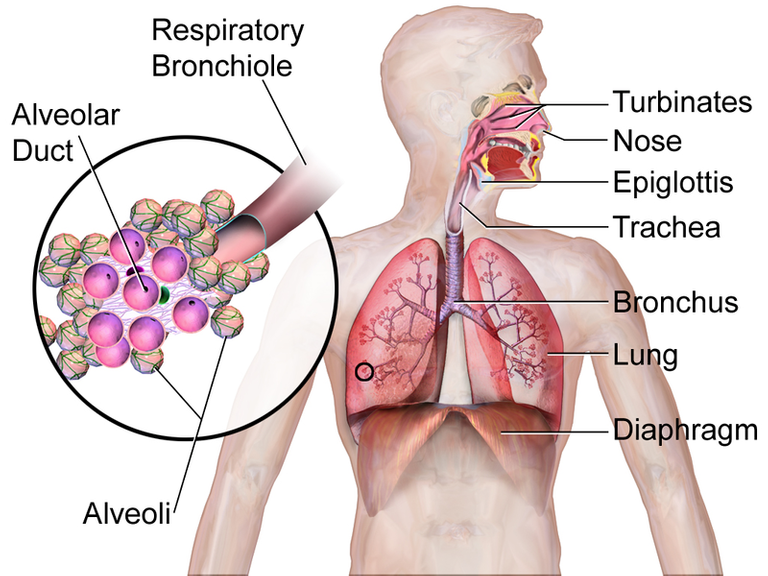
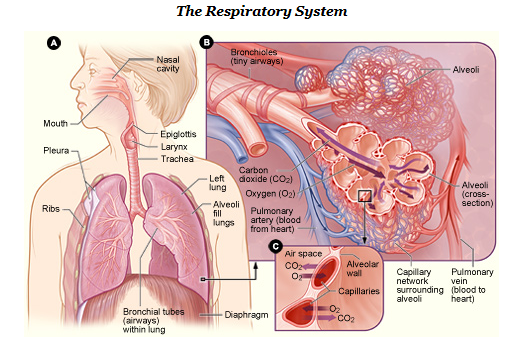
Stethoscope is essential in aiding physicians to come out with the possible diagnoses based on auscultation alone. Of course, the outcome of the breath sounds heard via the stethoscope alongside with proper history taking from the patient and the assistance of laboratory investigation will ultimately allow the physician to decide what kind of condition the patient is facing. The anatomy of the respiratory system is made up of several structures. It starts from the mouth/nose, pharynx and larynx. This is called the Upper Respiratory Tract. Many of you guys must heard or at least came across the written diagnosis of URTI. URTI means the Upper Respiratory Tract Infection. Bear in mind that even the infection of the ears and the nasal sinuses are considered as a type of URTI.
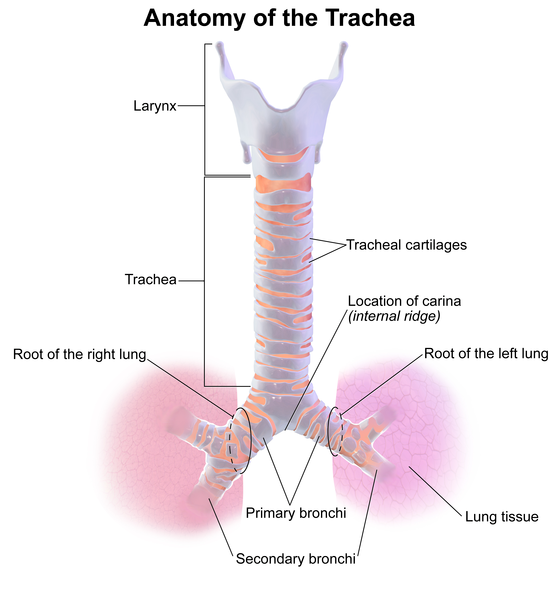
Auscultation in the respiratory system mainly involves the lower airways which are the Trachea, Bronchi and Bronchioles. The trachea is about 10-12 cm in length and it is slightly tilted to the right. Carina is the main division point of the trachea where it separates both bronchi. The right main bronchus, which is the pathway to the right lung, is more likely to be filled with foreign bodies such as nuts and marbles as the structure is more vertical compared to the left counterpart.
There are three lobes in the right lung and two lobes of the left lung. Lobe means small, rounded projections. These lobes are separated by fissures. The right bronchus divides into the upper lobe bronchus and the intermediate bronchus, which further subdivides into middle and lower lobe bronchi. For the left side, the left bronchus divides into the upper and lower lobe bronchi only. There are about 15 divisions in all between the trachea and alveoli. It is important to know and these structures either aids in the breathing process or protects the lungs from foreign materials.
The first seven division are bronchi parts which include the walls consisting of cartilage and smooth muscles, an epithelial lined by cilia and goblet cells, submucous-mucus secreting glands, and some endocrine cells. The next 16-18 divisions are called the bronchioles. They contain no cartilage, a single layer of ciliated cells but very few goblet cells and granulated Clara cells that produce surfactant like substance.
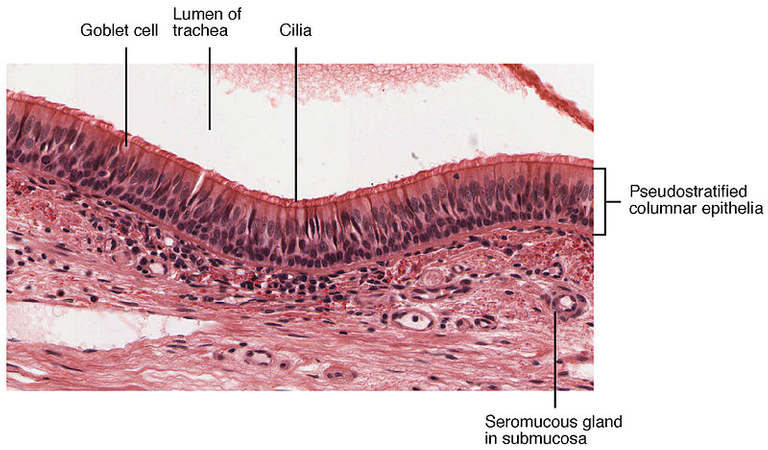
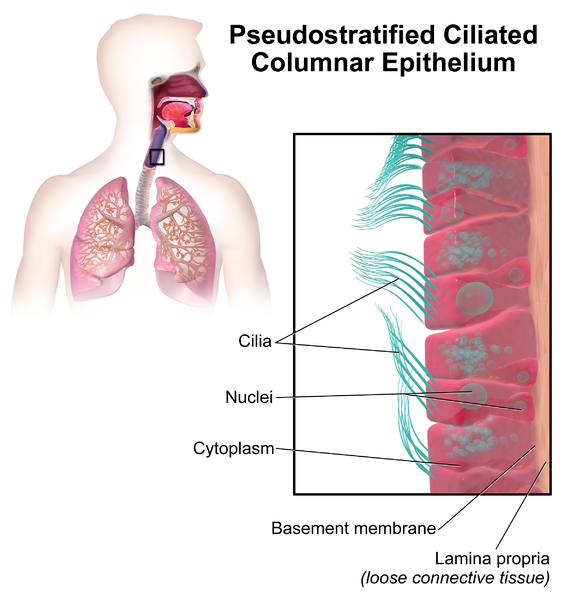
The cilia and goblet cells are the key defense mechanism of the lungs. Each cell bears almost 200 cilia. Cilia is the plural form of the word cilium, which means a short-microscopic hair-like vibrating structure on a surface of a certain cells. The cilia moves or beats at 1000 beats per minute in an organized waves of contraction. Each cilium consists of nine peripheral parts and two inner fibrils. These cilia move together to expel mucus, dead white blood cells, cell debris, any inhaled particles and bacteria out from the trachea.
The bronchioles subdivides into smaller bronchioles that have alveoli arising from it. Alveoli are grape-like structures which contain tiny sacs of air which allows rapid gaseous exchange. Each bronchiole supplies approximately 200 alveoli. Each lung has about 300 million alveoli to aid our respiration process. There are two main important Pneumocytes surrounding the alveoli. Pneumo means air/gas and cytes are cells. The epithelial lining of the alveoli consists of type I pneumocytes. These cells support gaseous exchange as they are very thin. Hence, oxygen and carbon dioxide can easily enter the blood stream from the alveoli. Type II pneumocytes are the main source of surfactant. Surfactants are compounds that lowers the surface tension between two liquids, gas and liquid or liquid and solid. They are lipoprotein complexes and the main substance inside is the dipalmitoylphosphatidylcholine (DPPC). Quite a long name huh.
They have three main functions:
- Increase pulmonary compliance (the ability of the lungs to stretch and expand)
- To prevent atelectasis (lung collapse) at the end of respiration
- Facilitate the recruitment of collapsed airway
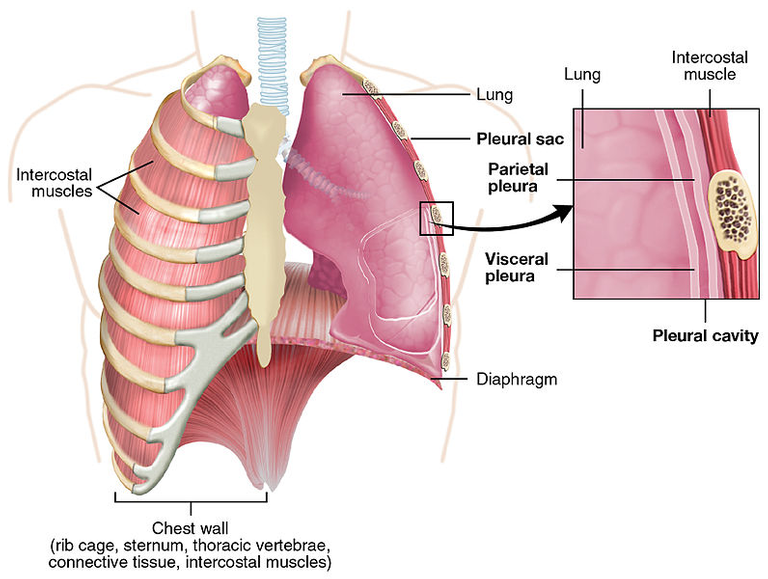
The pleura is a layer of connective tissue which is lined by a simple squamous epithelium. There are two types of pleura, namely the visceral and parietal pleuras. Viscera means internal organs, hence visceral pleura covers the main organ, which is the lungs. Parietal means relating to or denoting the wall of the body or of a body cavity or hollow structure, hence it covers the outer membrane of the lungs. It is important of know the existence of these two pleural layer as there is space in between these two pleura (pleural cavity) which can be pathologically filled with fluid or air. The diaphragm on the other hand is a sheet of skeletal muscles that aids the lung in respiration.
During the auscultation process, the patient needs to take deep breath through the mouth. The inspiratory phase should be longer than the expiratory phase. Normal breath sounds are caused by turbulent sounds in the larynx and in healthy lungs, the high-pitched component is filtered which results in the normal breath sound – vesicular breath sound.
Bronchial breath sounds
They are characterized by expiration and inspiration producing noise of equal loudness and duration. It is like blowing through a hollow tube. Similar sound can be heard in the trachea. Hence during the auscultation process, it is a good idea to compare the bronchial breath sound from the lungs and those from the trachea. This sound occurs as a result of abnormally increase in airway transmission to the surface of the chest.
Causes
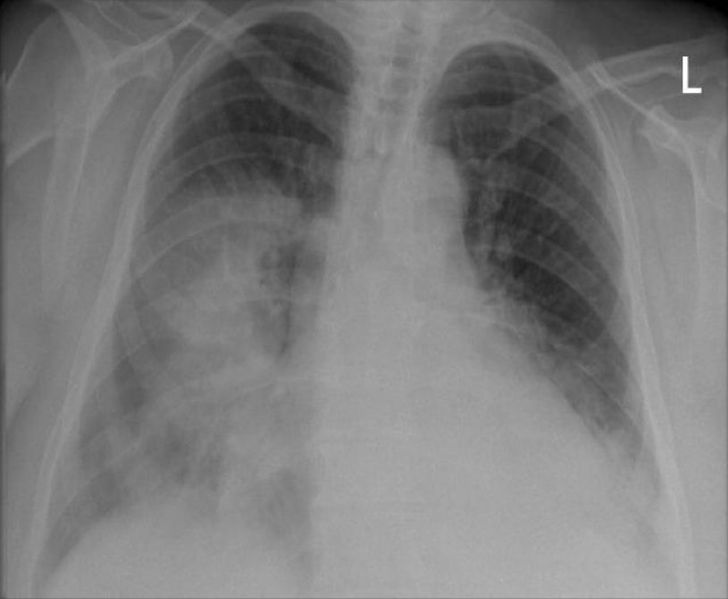
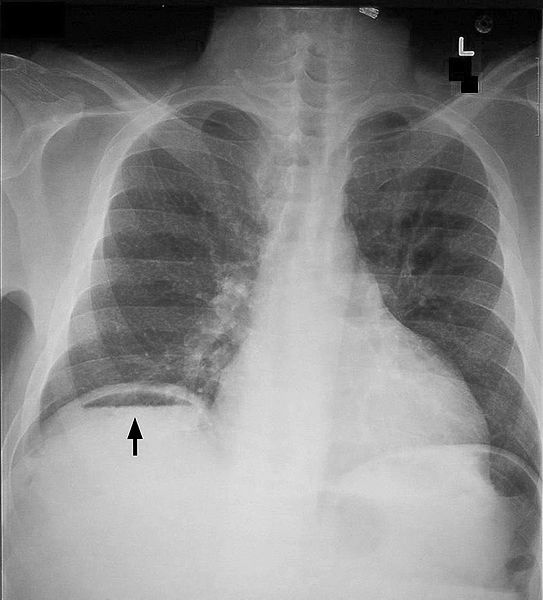
The commonest cause is consolidation. Pulmonary consolidation is a region of the lung tissue that is filled with liquid instead of air. The main culprit is the accumulation of inflammatory cellular exudate in the alveoli and the adjoining ducts. One of the famous cause of consolidation is pneumonia (infection of the lungs). Other causes of bronchial breath sounds are localized fibrosis and collapsed lung. Chest X-ray (PA view) above shows consolidation within the right mid and both lower lobes.
Added Sounds
Wheeze/Rhonchi
Generally, wheezing is the audible counterpart of rhonchi. Wheeze results from vibrations in the collapsible part of the airway as a result of limited air flow. It is most commonly heard during expiration and it could be monophonic (single large airway obstruction) or polyphonic (narrowing of many small airways). Asthma and COPD are the causes of wheezing.
Causes
COPD – Chronic Obstructive Pulmonary Disease

It is predicted to be the third most common cause of death and 5th leading cause of morbidity in the world by 2020. It is a clinical syndrome that comprises of airflow limitation and destruction of lung tissues. To compare it with asthma, the airflow limitation in COPD is typically not fully reversible. The cause of COPD is due to prolonged exposure of toxic particles and gases in which 90% of it comes from smoking especially in developed country. The small airways are affected in the early phase of the disease without any symptoms. In late stages, despite the absence of cigarette smoke, the ongoing inflammation continues. The physiological consequences of this condition is the airflow limitation. The characteristics of COPD are productive cough with sputum, wheezing, breathlessness and it usually occurs after years of smoking (even passively). I have seen a patient with COPD who does not smoke but passively inhaled her husband’s cigarette smoke for decades. The treatment is mainly to relief the symptoms such as by giving short acting B2- Agonist – Salbutamol and even long acting B2-Agonist – Formoterol or Salmeterol. Some patients can be better with the administration of steroids as it has anti-inflammatory properties.
Crepitation
These are brief crackling sounds produced by the opening of previously closed bronchioles. The closure of bronchioles can be due to collapse alveoli by fluid, exudates or lack of aeration during expiration. They are continuous, non-musical (wheezes are musical), and brief. They are often described as either coarse crepitation or fine crepitation. Fine crepitation usually occurs in late-inspiratory phase while coarse crepitation is during early inspiratory phase. Fine crepitation can be simulated by rolling a strand of hair between one's fingers near the ears. Coarse crepitation is associated with diffuse airway limitation such as in Bronchiectasis while fine crepitation is related to pulmonary edema and lung fibrosis.
Bronchiectasis
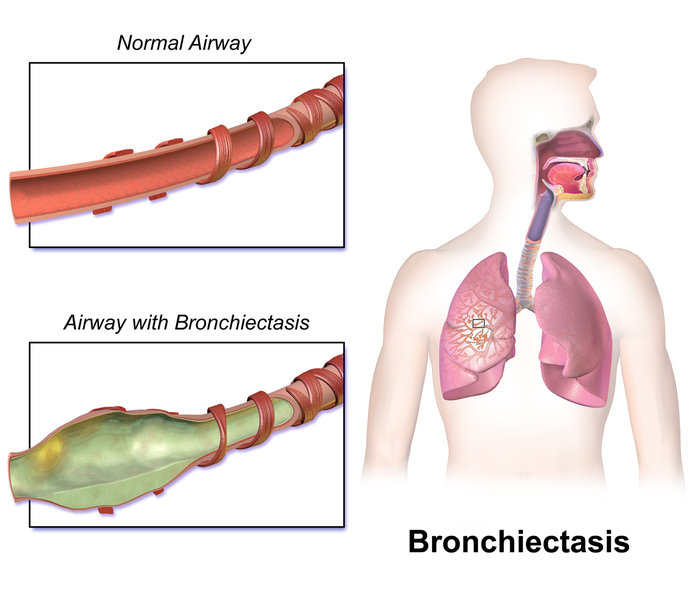
This is a condition often describes as abnormal and permanently dilated airways. The vicious cycle of inflammation and recurrent infection damage the airway. As a consequence, the ciliary movements are impaired which further aggravates the situation as the lungs are unable to expel unwanted materials from the lungs. Bronchiectasis is often associated with COPD. Individuals who suffer from Bronchiectasis will present with productive cough, breathlessness, infection symptoms, and even hemoptysis (coughing out blood). To confirm the diagnosis, High Resolution CT Scan is the best modality and the radiological imaging technique might show non-tapering ‘tram track’ airways and an increased bronchoarterial ratio ‘signet ring’ sign. Treatment-wise, it is recommended to expel the airway secretions via chest physiotherapy and debilitating the source of infection via antibiotics.
Gastro-Intestinal System
In this system, the main purpose of using the stethoscope is to listen to the bowel sounds. Increased in bowel sounds, high-pitched and tinkling in nature are highly suggestive of fluid obstruction. This is due to the movement of fluid in a dilated bowel. Absent bowel sound probably points towards peritonitis. Peritonitis is a serious condition which is described as the inflammation of the peritoneum (the lining of abdomen/abdominal organs). In cases of bowel obstruction, absent bowel sounds may suggest strangulation of bowel ischaemia.
Peritonitis
This condition usually causes severe pain resulting from the irritation of peritoneum due to infection or from chemical irritants caused by leakage of intestinal contents. E. coli and Bacteroides are the two most common organism involved in this situation. The inflammation produces exudates or pus that will spread throughout the abdominal peritoneum layer leading to intestinal dilatation and paralytic ileus. Ileus is the obstruction of intestine. Chest X Ray can be done to detect the condition. The findings via this radiological imaging technique include the free air under diaphragm. The treatment of this condition is by looking for the primary cause and some surgeries.
In a nutshell, stethoscope has many uses in the medical field as some life-threatening conditions can be detected by just listening to the chest or tummy. You do not have to run high tech and sophisticated laboratory investigations to all incoming patients to diagnose the condition as it will cost a fortune. Try to imagine that you need to do CT thorax to all patients that complain of breathlessness. Not practical at all. However, good clinical experience are required to master the diagnostic skills of using the stethoscope. Hence, it’s a good advice to start practicing if you want to be a doctor :)
References
- Kumar P., Clark M., Kumar & Clark's Clinical Medicine. Ninth Edition. London: ElSevier, 2017. Print
- What are the uses of stethoscope?. Healthfully. Retrieved on April 29, 2018, from https://healthfully.com/uses-stethoscopes-5104562.html
- How Stethoscope Works. Julia Layton. howstuffworks. Retrieved on April 29, 2018, from https://science.howstuffworks.com/innovation/everyday-innovations/stethoscopes1.htm
- Bronchial Breath Sounds- Introduction. Easy Auscultation. Retrieved on May 1, 2018, from https://www.easyauscultation.com/bronchial-breath-sounds
- Crackles. Wikipedia. Retrieved on May 1, 2018 from https://en.wikipedia.org/wiki/Crackles
- Peritonitis. Wikipedia. Retrieved on May 1, 2018 from https://en.wikipedia.org/wiki/Peritonitis
True, this is the primary tool used by doctor for their initial diagnosis and is very essential in the field of medicine. Great article @soulesque
Thank you for the support :)
You've been upvoted by TeamMalaysia community. Do checkout other posts made by other TeamMalaysia authors at http://steemit.com/created/teammalaysia
To support the growth of TeamMalaysia Follow our upvotes by using steemauto.com and follow trail of @myach
Vote TeamMalaysia witness bitrocker2020 using this link vote for witness