StemQ Notice: The following is an answer to this question
These are indeed very good set of questions. How do we know that the HIV is causative agent of AIDS? I will try to convince you that it is by pointing at the ample evidence and will try answer these questions.
Image sources:
HIV virus by BruceBlaus | CC BY-SA 4.0
AIDS by geralt | Pixabay
Let me start by requoting the list of the questions below?
>But how do scientists know that HIV causes AIDS, how reliable is that evidence?
Did they even try to identify this virus in people without AIDS symptoms?
How much people did they scan?
Is there any stronger evidence that HIV causes AIDS than just isolation (like an experiment)?HIV stands for human immunodeficiency virus. So, we can't use animals to make that experiment. Is that correct? Why exactly?"
-Questions by @alexbiojs
How do we know, if any pathogen is causative agent for a given disease?
A very old, yet elegant set of postulates come to rescue. Also known as the Koch's postulates.
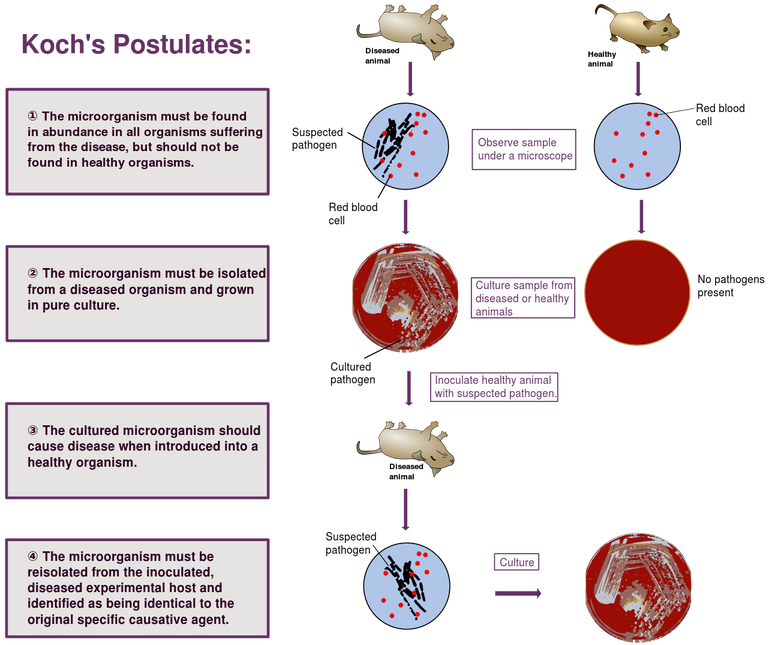
Koch's postulates
Image by Mike Jones | CC BY-SA 3.0
These postulates stated in the above image, are also in line with above questions. Which means that, if scientists have to prove that HIV, indeed causes AIDS, then they should -
Be able to show a significant correlation between presence of HIV and AIDS.
Be able to isolate and propagate HIV in lab from AIDS patients.
Inject the new healthy hosts with their lab grown HIV culture and replicate the disease symptoms.
Now, that we have the framework regarding what we should look for, we are better position to answer above questions. So let's start, shall we?
How do we know HIV->AIDS?
The finding that HIV causes AIDS was not free of hurdles. There were a lot of hypotheses were proposed to explain a set of symptoms observed in patients with AIDS. They included - fungi, bacteria, exposure to certain chemicals and even autoimmune disease targeting CD+ T lymphocyte (Gallo et al., 2003).
But, there were strong hints which sent people fishing for a viral agent, a retroviral agent to be more specific. The first hint was that AIDS was specifically characterized by depletion of CD4+ helper T-cells. Note, not any other T-cell subtype such as CD8+ T cell or gamma-delta T cell. This was a hint that something is specifically targeting CD4+ T cells. What made it clearer is that it can be transmitted, a lot like HTLV virus. Yet more interesting was the fact that it can be transmitted by blood transfusion of just clotting factors to hemophilia patients. This type of transfusion have no cells but just molecules and molecular assemblies, which hinted that causative agent can't be bigger than the virus. The second hint came from animal models, in which it was known that a lymphotrophic retroviral infection causes a similar phenotype. And hence the hunt for retrovirus began.
By 1984, they have isolated the virus and by 1985, an ELISA test which recognized HIV came into picture. These were initially called HTLV-III or LAV (Lymphadenopathy associated virus ), before they concluded that it was this same virus found in patients with aquired immunodeficiency, and called it HIV (see Gallo et al., 1985, Motagnier et al., 1984, Wain Hobson et al., 1991). By 1987 it was established that retrovirus is present and can be isolated from high percentage AIDS patients and patients showing AIDS related symptoms (Casareale et al., 1987).
This was then followed by decades of tests and in fact made HIV presence a diagnostic criteria for AIDS. So if you have decreased CD4+ T-cells count, increased incidence of oppurtunistic infections and if you are HIV+, you diagnosis will be AIDS. And in almost all cases of symptoms matching AIDS, the patients have antibodies against HIV virus. But is it possible to have AIDS like symptoms and be HIV negative? The answer is yes.
For instance, if you have symptoms similar to AIDS, along with decreased counts of CD4+ T-cells, but you are HIV negative, and no other immunodeficiency or adverse effects of some drugs, you probably have a rare condition known as Idiopathic CD4 positive T-lymphocytopenia (ICL). Even though ICL and AIDS share similar etiology and consequences, they have subtle differences, nonetheless (Mukherjee et al., 2009). Such as no apparent rise in CD8+ T-cells, plus the declined CD4+ populations remain stable even without anti-retroviral treatment. Moreover AFAIK, there have been no reports of ICL being infectious. However, this doesn't mean that this rare condition disproves HIV-AIDS link. It rather shows that if you kill CD4+ cells either because of some condition or because of viral infection you may produce more or less similar symptoms. Moreover, since HIV capability of killing CD4+ T-cells is well known (Cummins and Badley., 2014). So what we are seeing here is a common pathway to leading to similar symptoms. In one case a virus killds CD4+ cells and in another some genetic or epigenetic defect may achieve the same.
However, do all HIV virus carrying individuals develop AIDS? What about using purified cultures to infect new hosts?
Do all HIV+ people develop AIDS?
The answer is no! Now one may ask then how can we conclude that HIV, causes AIDS. The answer lies in long latency periods of HIV virus. As it turns out, one may get infected with HIV. The virus will just go and insert its genome in T-cells and continue replicating without making a lot of noise. However, it would be visible in PCR tests, nonetheless. It can stay like that for decades and in some cases latency may even outlive the person (see Medley et al., 1987). The HIV-2 virus, have even longer asymptomatic period. The icing on the cake are long term non-progressors. Some genes provide high immune protection against HIV in these people. An example of such a protective gene variant HLA B27. These people can get infected with HIV but may not develop AIDS (den Uyl et al., 2004). To say the least, these protective mechanisms immunologically targeting HIV to delay onset of AIDS, post HIV infection, are rather pro HIV-AIDS casual relationship.
The accidental and experimental evidence.
Till this point we saw 1st two Koch's postulates being fulfilled. That is HIV is correlated with AIDS and can be isolated and cultured from these patients. But what about the third postulate? Can these pure cultures cause infection in healthy hosts?
Well of course, as mentioned in the original question, it would be unethical to inject a deadly virus in healthy humans. But sadly, there have been some tragic lab accidents in which researchers were exposed to purified virus. These researchers did contract AIDS and HIV virus was isolated from them and shown to be the lab isolated strain (Sipsas et al., 1997, O'Brien et al., 1996).
Can HIV infect other animals?
HIV is mostly specific to humans, this is because every virus has a specific receptor on cells that it recognizes and uses to bind and gain entry into the cells. How many species a virus can infect hence depends on what all cell surface receptor can it bind to and how sequence homology for this particular receptor is there between species. The gp120 on surface of HIV virus interacts with CD4 receptor on T-cells and another co-receptor such as CCR5 to gain entry (Clapham et al., 2001).
Given the above information, the most likely animal that you may predict to get infected by HIV is chimpanzee. Though chimpanzees have evolved mechanism to not progress to AIDS by HIV or their own version of virus - SIV. Hence, many infected chimpanzees remain long term non progresses, however some of them do progress to AIDS via HIV infection (O'Neil et al., 2000). Moreover, the primate cousin of HIV, the SIV virus (also thought to be ancestor of HIV) can also causes AIDS in other primate species. In fact, you can even use the cDNA genome of SIV virus cloned in a plasmid and infect rhesus macaques using this plasmid (Liska et al., 1999, Baba et al., 1999). The macaques will eventually progress to AIDS. You can isolate HIV-2 from humans and infect baboons with it. The infected baboons develop AIDS like disease and some of them even succumb to a fully fledged AIDS (Locher et al., 1998). In yet another experiment done in 1996, Jaog et al., , made a chimeric virus, with envelope gene of HIV and gag and pol genes from SIV. By doing so, they successfully demonstrated infection and development of AIDS in macaques by this chimeric virus. Last but not the least, Aldrovandi et al., 1993, demonstrated that HIV infection and the process of its pathogenesis can also be demonstrated in immunodeficient SCID mouse, implanted with human thymus (organ where T-cells mature).
In the light of above mentioned evidence of lab accidents and animal models, we can say with confidence that HIV- AIDS association satisfy Koch's postulates. The evidence is pretty strong and has been tested over and over in the decades. Moreover given the fact that anti-retroviral drugs have ability to delay the progression to AIDS in HIV+ people, and significantly reduce morbidity and mortality, we can say that we also have drug inhibition related evidence for this association (Rodger et al., 2013, Nakagawa et al., 2013).
I would like to close the write by saying, that AIDS is not one disease, but a a condition caused by severely compromised immune system lacking CD4+ T-cells. The morbidity and mortality in AIDS rely not on HIV but on all the secondary infections it makes you prone to. Given this similar immunocompromised conditions, such as - ICL, sarcidosis, and other genetic immunodeficiencies may present similar features. However, for the purposes of the trasmissiable viral immunodeficiency that is of concern to this question - HIV-1 and HIV-2 are the causative agents.
References
Gallo and Montagnier, 2003. The Discovery of HIV as the Cause of AIDS
Mukherjee et al., 2009. Idiopathic CD4+ T-cell lymphocytopenia
O'Brien et al., 1996. HIV causes AIDS: Koch's postulates fulfilled
Clapham PR, McKnight A. HIV-1 receptors and cell tropism. Br Med Bull.
O'Neil et al., 2000. Progressive Infection in a Subset of HIV-1—Positive Chimpanzees
StemQ Notice: This post was originally submitted on StemQ.io, a Q&A application for STEM subjects powered by the Steem blockchain.
I like the concluding paragraph, some think of AIDS as one disease. This was pretty detailed. Also interesting is the chimpanzees reference and some of the group that their SIV does not progress to AIDS, I think we have the same parallel in human as seen in some people from the Northern Europe.
Ah! The CCR5 mutation. Some of them are even resistant to getting infected by HIV in first place. It would be interesting to know which primates have if any have a mutated CCR5 selection in past. That could provide a good animal model to understand how this pathway works and develop drugs that can protect all humans from HIV infection. Or we can create the animal models with this mutation
Chimpanzees, however are also known to have gone through a selective sweep in their HLA repotire. This has indeed a lot to do with the long term human non progressors with HLA B27 and B57 variant.
Thanks for reading and your feedback. It always motivating to have discussion in comments of the post.
This is a time that I actually envy people with mutations :)