I read something about proposal #332, I went on #PeakD and clicked on the support buttons, I hope that was the vote, if not let me know what I have to do. #leo2025
midnight here but I can't sleep due to high #fever and #flue, now i took tablets so that i can sleep peacefully..... The #Panadol is the only tablet which i took it in such kind of emergency 😕
i don't have plans to withdrawal my cryptocurrency so I think bull run doesn't affect me so far but yes I'm happy to see the increasing vote value on hive 😀
Agreed we need to try something different and commenting and engaging on Hive blog posts does not help us.
We need to move all the activity here to InLeo.
Leave those accounts in a barren wasteland of auto-upvoted posts.
I'm not surprised. I brought a follower over from the Arena who has 20,000 followers on DeSo and he made a test post and was immediately downvoted which neutralized my vote. Needless to say he wasn't too exited about HIVE.
I hear you. There are some people on Blurt and Steem that don't post on HIVE because of the flagging wars and some of the guys in Discord were just laughing at new users that they downvoted into the ground right as they joined. It's weird stuff for sure.
Just early investors/holders of Steem/Hive. Every project has growing pains and the early community sometimes wants to keep things small so they're more important.
Your support and is invaluable. I'm working hard on the back-end to make it more attractive for more people to use, and really appreciate how you've been working the "front-end" to spread the word and engage people
Yes. Hopefully this new ability to present the numbers, along with much more detailed daily reports will make it more attractive for some to contribute. Then we keep adding incentives-I have plans!
all that you do on the platform is just helping it grow so well. Wishing for more progress. And I can't imagine how much data we'll get from this in 2025
You are welcome to the Blockchain my dear friend, please feel free to roll around and have more fun are we grow our reputation on the Blockchain. Welcome to the jungle my dear, you are now a kitten, I hope you grow to become a full lion..
I lived for 8 months in a inner city of Ireland, and I backpacked for 2 months around Europe (I visited 15 countries) and I never ate (nor did I see other people eating) pork. 🤔
Trump speaks about acquiring other countries through different means and his own country is burning. I hope he wakes up and really take care of his own people.
Usually it is more than one cause - unusually bad weather, poor forestry, building homes at the worst place possible, lack of water in hydrants, incompetent people in charge etc.
I can read one line very fast, but I'm on the slower-end if you look at how long it takes me to read a book. I love to ponder while reading, I usually spend 10x the time reading a page, pondering or re-reading some parts. #mydiary #cent #bbh
We should be proud because not everyone has the beautiful house that we have. Our platforms are better than Facebook or YouTube. While the big social networks profit from people, Inleo and Hive are betting on incentivizing creators.😎
i thought YouTube had already overthrown Facebook. Hive is built like a Blockchain Facebook so it's potential is billions of users woaw when it happens one Alfa will be mega popular 🔥
True. We have the infrastructure that supports this growth (Hive blockchain), we just need more social media apps that are booming like InLeo. We shouldn't reside on a single app to do the hard lifting.
clearly team work to bring in the adoption is needed. Great stride were made by the team behind Leo and the community last year. Looking forward to even bigger bolder strides in the year present.
I'm not to old here but it's a wonder why Hive ain't like on top because people keep posting on Facebook which controls everything they do and they earn nothing. Are we getting limited in promotion
In 2014, Californians overwhelmingly voted to spend billions on water storage and reservoirs.
Gavin Newsom still hasn’t built it.
Now no water is coming out of the fire hydrants.
Camera man spotted inside the shot, did they just said, fuck it who is going to notice...or is it part of the series? 😅🤔
#skiptvads , #squidgame , #netflix , #tvonleo
Only fans will spot such things. I had that so many times on sets where I was involved. I even called out the DOP on it when I was next to him. His answer: If they spot it, they are big fans of the show...
Maybe you have not reached the threshold yet.
But sometimes it is just a display bug.
Whenever you feel something is wrong with the site use #feedback so the team can check on it.
Carry On (2024) was good although how does it turn into one of Netflix most popular movies of all times? there were times I almost shutit down, is not that great but its entertaining 🤔
#skiptvads , #moviesonleo , #netflix , #carryon2024
I would say Taron Egerton character felt shallow, like he was everyone btch besides having a bossy girlfriend, like he was never in control of the movie
"Carry On" has climbed the Netflix charts, becoming one of the most popular movies on the streaming service, the film's success can be attributed to its engaging storyline and the performances of its cast, viewers are enjoying the mix of humor and heartfelt moments, making it a standout in Netflix's current lineup, Read More in ➡️ #linkincomments
2/🧵You can help to keep this trend alive by voting for the latest DHF Proposal to allocate 0.56% of the Daily Budget for INLEO to fund the marketing collaborations made with other Keystore supported projects such as BTC, ETH, RUNE etc.
Goldshell Mini Doge III - Gets 700 MH/s at 400W in full go mode and 550 MH/s at 260W in low power mode. Perfect for a small off-grid solar setup. I can run 3-4 miners on this one PSU.
Yeah, next step is to buy the solar panels, charge controller, batteries, and inverter I need. LOL. But it's not that bad. Going to run on grid until I get the solar all built.
I haven an old miner that uses mining specific GPUs. (nvidia GTX 1060 equivalents). Not useful for mining these days but still ok on Einstein@home. I got a server power supply and breakout board. Sometimes cheaper and a lot more reliable.
Yeah, I thought about getting a mining rig going because I have a couple of older RX580s and 480s that I would at least like to stick on Ravencoin, but not sure if it's worth it these days. Sill might in the future, but I am liking the specs on these DOGE/LTC miners.
A Rich and well documented history.A major key why another group of people would assume themselves more superior than others, who hardly know a thing about there passed making them repeat the same mistakes and not have nothing to build on.
Entrando a Hive, quiero compartir con ustedes mi pasión
#bqto
Hola amiga, bienvenida a esta gran mundo de Inleo, donde podrás conseguir grandes resultados y pasarla muy bien.
Check out this video where our dev talked extensively about Gifu and crypto news.
#gifu #crypto
Wait... Gifu is not just a HIVE token?!
yeah, Gifu is built on Binance Smart Chain.

on it...
There's currently only 69 players on Crownrend.. I'd say that still counts as early..
Care to join? - https://crownrend.com/?ref=MEMQNPWK4THTC
Friendly reminder.....Only if you wanna have an epic 2025 on $LEO
thanks for this advice, I'm going to follow through it
Easy plan.
The best thing I have read all day, knowing I am slowly learning how to participate in the community. Thanks jongo, this is on point.
thanks for checking it out, glad it was of value :)
thanks for the timely reminder
I read something about proposal #332, I went on #PeakD and clicked on the support buttons, I hope that was the vote, if not let me know what I have to do. #leo2025
Thank you for supporting INLEO! Leave a positive comment on their blog post too
Ok, I did vote correctly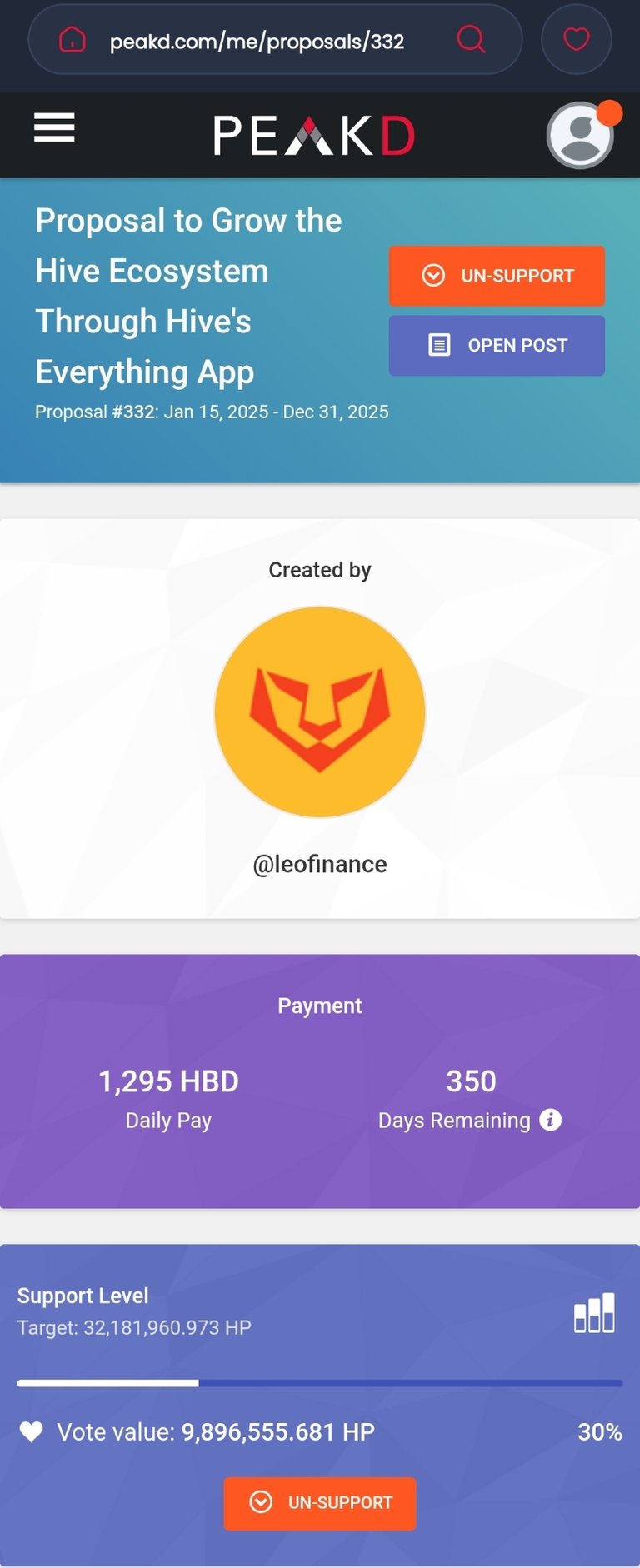
#leo2025
midnight here but I can't sleep due to high #fever and #flue, now i took tablets so that i can sleep peacefully..... The #Panadol is the only tablet which i took it in such kind of emergency 😕
#Hive #leofinance #threads
Good photo my fren! Keep Creating content :))
My first post 🙋♀️

Welcome to InLeo!!
Glad to have you here!
Bienvenida Mava 🙌🏻🎉😅
#gmfrens
It's Thursday, 9 January 2025
Today's #lbi asset backed value per token is:
1 LBI = $0.234 USD = 0.419 HIVE = 3.990 LEO
Have a great day everyone.
♦️ You got 0.01 FELT for sharing high vibes on Hive.
📋♦️ FELT Info
i don't have plans to withdrawal my cryptocurrency so I think bull run doesn't affect me so far but yes I'm happy to see the increasing vote value on hive 😀
#Hive #leofinance #threads
a top 20 witness tried telling another top 20 witness what they can and not post due to it draining the reward pool.
This happened today.
They only care about how much they are making not growing the chain.
If you want InLeo / Hive to grow stop following their curation trails. Stop auto-voting trending posts. Stop giving them your proxy votes.
Come to InLeo and build a community and use all your power to support each other.
Amen
I agree with this. We tried to build Hive a certain way for a long while. Lets try the Lion way now 🦁🥂
Agreed we need to try something different and commenting and engaging on Hive blog posts does not help us.
We need to move all the activity here to InLeo.
Leave those accounts in a barren wasteland of auto-upvoted posts.
I'm not surprised. I brought a follower over from the Arena who has 20,000 followers on DeSo and he made a test post and was immediately downvoted which neutralized my vote. Needless to say he wasn't too exited about HIVE.
That just pisses me off. I'm about to start taking names and making visits. I'm from a different era ;-)
I hear you. There are some people on Blurt and Steem that don't post on HIVE because of the flagging wars and some of the guys in Discord were just laughing at new users that they downvoted into the ground right as they joined. It's weird stuff for sure.
yeah Hive is a waste of time. InLeo and earning Leo is the future.
where does all this juicy stuff happen? lol
i only hang out in Threads....looks like I miss out on the fun lol
private backroom chatrooms.
it is kind of disgusting TBH. but I dont want to lose access.
This is why I say I don't even like discords for projects / games etc...
just build everything in public and talk in public.
Hi, @simplegame,
This post has been voted on by @darkcloaks because you are an active member of the Darkcloaks gaming community.
Get started with Darkcloaks today, and follow us on Inleo for the latest updates.
♦️ You got 0.01 FELT for sharing high vibes on Hive.
📋♦️ FELT Info
I guess it's all the old guard over on Peakd and Ecency. They don't like Inleo anyway, they think we are the stinky kids, lol.
I'm glad to be a stinky kid!!!! lol
Small mind thinking. Where we're going, everything is 100x bigger.
Grow grow grow, leave the anti-growth in the dust.
yep that is why I never go to HiveFest. Too much of them.
Over the year I have had my fill.
We will outgrow them 100 percent !!!!!!
Interesting! I had a good experience because I didn't know who the trolls were to look out for.
yeah it can be a good time. They put on the masks for sure.
But once you learn more things change. I have so many stories.
Feel free to DM if you get any spare time to kill, I love gossip 😆
will do. I have stories for sure.
We need a US based LEOFest! I'll DJ, lol.
I can make it happen, a local DashFest with LEO folks invited.
agreed.
as long as we could get Khal to leave Chicago.
Exactly! Where we're going we don't need whales.
So who are these people? I'm starting to see more and more talk about this on threads
Just early investors/holders of Steem/Hive. Every project has growing pains and the early community sometimes wants to keep things small so they're more important.
Hmmm I see
Name names so we can unfollow/unvote...
I cover this info on my subscriber only content.
#leaderboard Snapshot – January 8, 2025
for the YTSummarizer #aisummaries
This is pretty cool 👏👏👏... We need to keep it up...
Solid 2nd place! 💪
I need to feed more and increase my engagement...
Today was so busy with onboarding activities...
You're doing great. Can't do everything all at once :)
Smile 😊😊😊😊..
♦️ You got 0.01 FELT for sharing high vibes on Hive.
📋♦️ FELT Info
Need to add a great deal more.
Hi, @taskmaster4450le,
This post has been voted on by @darkcloaks because you are an active member of the Darkcloaks gaming community.
Get started with Darkcloaks today, and follow us on Inleo for the latest updates.
Oh yes sir, I will improve from my end..
Lets keep adding and expanding the number of people using the tool. Just imagine the numbers we could produce 🦁
Your support and is invaluable. I'm working hard on the back-end to make it more attractive for more people to use, and really appreciate how you've been working the "front-end" to spread the word and engage people
Your work is important and I just wanna try to showcase and make people realize it 🦁
by the way, did you see the new daily report format?
Yeah the new format is awesome!🦁🦁
Very nice. We need to keep promoting the idea.
Yes. Hopefully this new ability to present the numbers, along with much more detailed daily reports will make it more attractive for some to contribute. Then we keep adding incentives-I have plans!
Very good. I am looking forward to being able to simply add a channel and get what was posted and what wasnt. Should speed things up.
Yes the planned new front-end will be a game-changer. It's also my top priority. These latest changes lays the foundation for it.
the next mark Zuckerberg pending, keep writing them codes ❤️🔥
all that you do on the platform is just helping it grow so well. Wishing for more progress. And I can't imagine how much data we'll get from this in 2025
What is this about? Sorry to be an ignoramoose on this, lol.
No worries! I discuss it pretty thoroughly in my latest blog post, but here is the short version:
https://inleo.io/threads/view/mightpossibly/re-leothreads-cjhbc6ka?referral=mightpossibly
It was also the topic of the latest @cttpodcast episode, if you want to dive a bit deeper
♦️ You got 0.01 FELT for sharing high vibes on Hive.
📋♦️ FELT Info
em' as a #newlion @kamkam2014 I'm here to light 💡up this space
Welcome to InLeo!!
thank you
Thank
You are welcome to the Blockchain my dear friend, please feel free to roll around and have more fun are we grow our reputation on the Blockchain. Welcome to the jungle my dear, you are now a kitten, I hope you grow to become a full lion..
#freecompliments
Welcome to Inleo!
Damn wish I had some more money to throw into $RUNE right now 🤩
Didnt think I would see these prices again!
I missed the train to $rune 🥲
for a quick second I read that as 0.45 and I was freaking out.
hahahah!
Is $rune the next Bitcoin ?
Heading for 1000 staken BBHO! #bbh #cent #inleo
Awesome Fracking Sauce :) !BBH !DOOK !PIMP
That's a win!!
@bradleyarrow likes your content! so I just sent 1 BBH(29/100)@pele23! to your account on behalf of @bradleyarrow.
(html comment removed: )
)
♦️ You got 0.01 FELT for sharing high vibes on Hive.
📋♦️ FELT Info
On the bright side, Meta doesn't own the 2nd entry in the list: Youtube!
https://inleo.io/threads/view/onealfa/re-leothreads-kxskvrvg?referral=onealfa
oh yeah!
BITCOIN crashing. Great news. I continue buying #bitcoin because #bitcoin crashing means Bitcoin is on sale. #cent #crypto #bbh
Remember “Buy low….and HODL.” - Robert #kiyosaki
Less than 2 million more Bitcoins to be mined.
#bitcoin exchange balances shows positive sign...!
If you play games. Why do you play them?
What makes you come back to one game over another?
Beef and pork feed many, one takes longer to produce and raise to maturity as compared to the other. However the goal is to eat them in moderation.
The best legume is pork - there is this saying in my country. 😆
Funny, how chickens have been out classed when they are produced and processed in days and are the main food at fast food chains
I like eating beef with chesse :)
🚀
Really?!
I lived for 8 months in a inner city of Ireland, and I backpacked for 2 months around Europe (I visited 15 countries) and I never ate (nor did I see other people eating) pork. 🤔
Chicken will probably rank number one in USA if not then I don't know nothing about culture 😂
The winner without a doubt is pork. It is impressive that so many countries like it. Very interesting fact.
I like beef the most!!!
♦️ You got 0.01 FELT for sharing high vibes on Hive.
📋♦️ FELT Info
Only legends can relate...
#legends #funny #it
Haha this is funny 🤣
there’s no place like localhost 💪🏼🦁👍🏼
I want one!
You made me laugh and make me think this meme. 🤭
Simply shocking...

Meanwhile... Trump is thinking of ways to steal other people's territories.
Yeah. Let's Make American Great Again.
Trump speaks about acquiring other countries through different means and his own country is burning. I hope he wakes up and really take care of his own people.
all of America needs to wake up very fast
There are a lot of people on #hive that live around... hopefully everyone's safe.
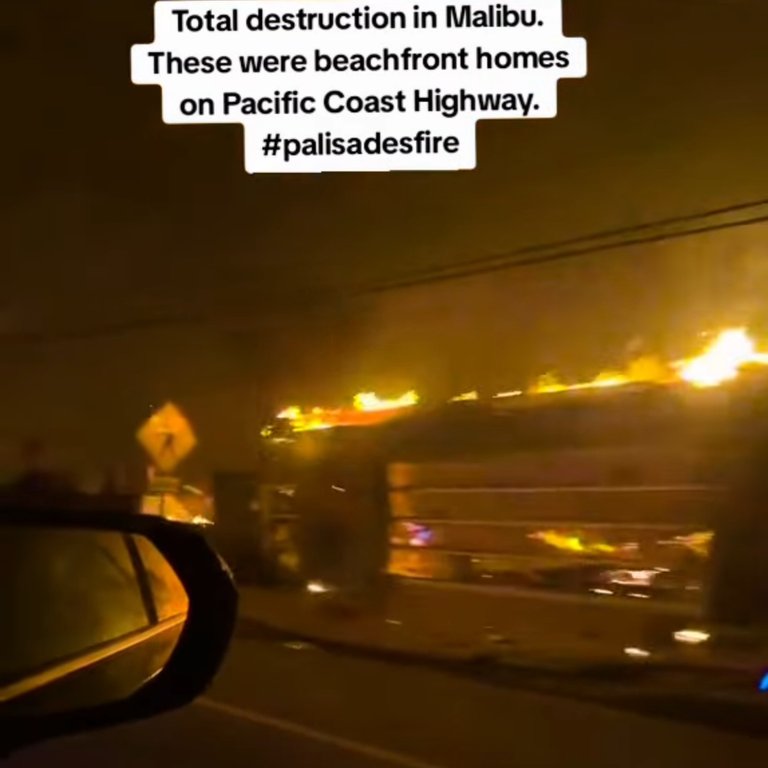
But before... Why was the destruction caused in Malibu?
Usually it is more than one cause - unusually bad weather, poor forestry, building homes at the worst place possible, lack of water in hydrants, incompetent people in charge etc.
This is shocking news, I will go read some more on Google!
how did this even happen 😳😳😳
I hope the government have started doing something about this 😱😱😱
Good show and introduction to Dash in 2025, Evolution, the DashPay wallet, INLEO partnership, and more!
The word is starting to spread.
Strap in for a great comeback year! 🔥
#dash #crypto
I'm Ready!!!
We'll get everyone living on Dash before you know it!
Dash is ready for the world 🔥
Yes! This year will really be eye-opening.
I can read one line very fast, but I'm on the slower-end if you look at how long it takes me to read a book. I love to ponder while reading, I usually spend 10x the time reading a page, pondering or re-reading some parts. #mydiary #cent #bbh
INLEO and HIVE have a large space to grow:

We do! I know there are a lot of issue with all of these sites. Hopefully we can find ways of NOT making the same mistakes they are.
We should be proud because not everyone has the beautiful house that we have. Our platforms are better than Facebook or YouTube. While the big social networks profit from people, Inleo and Hive are betting on incentivizing creators.😎
We are at the right place!
Thats an eye opener statistics. Is there data of active users for Hive and inleo?
I agree. Just look at those users waiting to be tapped and switch to web3.
There is room for growth and it has alot of potential
Facebook is a databroker, no like me this plataform!
That's a depressing chart...
i thought YouTube had already overthrown Facebook. Hive is built like a Blockchain Facebook so it's potential is billions of users woaw when it happens one Alfa will be mega popular 🔥
I pray one day it becomes a giant company, scratch that it won't be called a company and that's the best part
True. We have the infrastructure that supports this growth (Hive blockchain), we just need more social media apps that are booming like InLeo. We shouldn't reside on a single app to do the hard lifting.
very larger space indeed, imagine value of $LEO AND $HIVE when they even get to Pinterest level
Ahh! I guess we should start by comparing inleo with web3 media to gauge progress. We need long time to compete with web2.
clearly team work to bring in the adoption is needed. Great stride were made by the team behind Leo and the community last year. Looking forward to even bigger bolder strides in the year present.
And what’s makes it fun is Hive and inleo have the heart and courage to charge and merge victorious when Web2 comes tumbling down.
just capturing 0.5% of these users would be amazing. Long way to go but not impossible.
and so does #gifu
I'm not to old here but it's a wonder why Hive ain't like on top because people keep posting on Facebook which controls everything they do and they earn nothing. Are we getting limited in promotion
♦️ You got 0.01 FELT for sharing high vibes on Hive.
📋♦️ FELT Info
Crazy
Realmente eh realizado trading eficaz desde tribaldex y puedo sencillamente decirles que vale mucho la pena todo esto!! #spanish #tribaldex 🚀
Es una gran herramienta
Only fans will spot such things. I had that so many times on sets where I was involved. I even called out the DOP on it when I was next to him. His answer: If they spot it, they are big fans of the show...
Nice blooper 😅
hahaha

♦️ You got 0.01 FELT for sharing high vibes on Hive.
📋♦️ FELT Info
I have registered about 3 person, but I can't claim my rewards. Trying to claim will show successful, but when I check my wallet, I can't find them
Maybe you have not reached the threshold yet.
But sometimes it is just a display bug.
Whenever you feel something is wrong with the site use #feedback so the team can check on it.
what's the threshold for referral earnings withdrawal ?
I think it is 10$
It is entertaining, mostly because the side characters are well cast and good actors. The main character is a bit ... shallow, undeveloped? IDK
I would say Taron Egerton character felt shallow, like he was everyone btch besides having a bossy girlfriend, like he was never in control of the movie
It's something you can watch every Christmas season. I remember doing it for Die Hard and Lord of the Rings series. 😀
Revisiting the price of Runes. Will it be worth getting one in 2025? Or is a legendary plot better? #play2earn #hive #crypto #cent #bbh #inleo #splinterlands
#splinterlands
NASA's Vehicle Assembly Building in 1986. For scale, each stripe on the flag is big enough to drive a bus on.
#NASA #VAB #cent #bbh
I really like writing about NASA bro!
I have never asked AI to create a picture. Today I gave a first try
The design was very good and it looks a bit like you.
You (I mean, AI) did a good work.
Man, that's quite cool. Even AI knows about ONE ALFA. 😆
i also never use of Ai in making picture of words
Which tool did you use to create the image? Good morning!
chat gpt on my android phone
Fine my friend.
This is nice, I'll also try creating my own though my name will fuck up the AI 😂
Nice job you did a very good job in creating an image that looks so beautiful
"Carry On" has climbed the Netflix charts, becoming one of the most popular movies on the streaming service, the film's success can be attributed to its engaging storyline and the performances of its cast, viewers are enjoying the mix of humor and heartfelt moments, making it a standout in Netflix's current lineup, Read More in ➡️ #linkincomments
#carryon, #netflix, #streaming, #moviesonleo, #skiptvads, #randommedianews
Surprisingly good Christmas action movie in the mold of Die Hard 😀
Read More: https://screenrant.com/carry-on-2024-movie-netflix-most-popular-list-streaming-charts/
#skiptvads
♦️ You got 0.01 FELT for sharing high vibes on Hive.
📋♦️ FELT Info
1/🧵INLEO was the king of onboarding for 2024
INLEO solved onboarding by making any Keystore wallet compatible with #hive making new account creations go up by 4X.
29.69% of all new accounts were created by INLEO!
#threadstorm #outreach
2/🧵You can help to keep this trend alive by voting for the latest DHF Proposal to allocate 0.56% of the Daily Budget for INLEO to fund the marketing collaborations made with other Keystore supported projects such as BTC, ETH, RUNE etc.
3/🧵If INLEO does not manage to reach 50K MAUs, the funds received from DHF will be returned.
https://inleo.io/@vimukthi/hive-has-the-trading-volume-of-a-top-10-crypto-while-inleo-grows-exponentially-towards-50k-maus-hyh
Hey hey hey, dr. Lobes is in the house! @drlobes it has been a while! Where have you been?
Cheers mate...

Does he stake gold pressed latinum?
What's the rate from $HIVE,$LEO,$HBD to gold pressed latinum?
!LOLZ
lolztoken.com
He was resisting a rest.
Credit: reddit
$LOLZ on behalf of ben.haase
(4/10)
PLAY & EARN $DOOM
@forkyishere, I sent you anoh. The Ferengi. I love those guys.
Aviation Threadcast - Part 2
Here is a #threadcast about #aviation - incidents and accidents involving #airplanes
!summarize #aviation
!summarize #aviation #accidents #incidents #airplanes
Hi, @mightpossibly,
This post has been voted on by @darkcloaks because you are an active member of the Darkcloaks gaming community.
Get started with Darkcloaks today, and follow us on Inleo for the latest updates.
♦️ You got 0.01 FELT for sharing high vibes on Hive.
📋♦️ FELT Info
!summarize #aviation
!summarize #aviation
!summarize #aviation
!summarize #aviation
!summarize #aviation
!summarize #aviation
!summarize #aviation
!summarize #aviation
!summarize #aviation
!summarize #aviation
!summarize #aviation
!summarize #aviation
This channel is just so good! They're all worth watching to be honest. But now we have them summarized on Hive as well.
Now the videos are immortalized on the Hive blockchain.
They sure are
Hi, @coyotelation,
This post has been voted on by @darkcloaks because you are an active member of the Darkcloaks gaming community.
Get started with Darkcloaks today, and follow us on Inleo for the latest updates.
♦️ You got 0.01 FELT for sharing high vibes on Hive.
📋♦️ FELT Info
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
!summarize #aviation #accidents #incidents #airplanes
this is good, so much to learn from them. I don't get flight sickness though, afraid of heights
♦️ You got 0.01 FELT for sharing high vibes on Hive.
📋♦️ FELT Info
If you vote for LEO proposal this line keeps going up 🚀
We're on track to 50K MAU with new communities from keystore onboarding 📈
Link is down in 🧵
https://peakd.com/me/proposals/332
InLeo is the biggest onboarding on Hive, of course I will vote again for their proposal.
Imagine this Guy at your back door!? 😱#meme #photographers
He's a goner 🤣
!DOOK
he just needs a good petting
Mr. Carter made history.
Awesome INFO!
Quite longeviv presidents. I was expecting due to stress to live less than the common citizen.
U.S. Presidents sure do live a long time. Even before people knew much about health care.
Wow! Jimmy Carter I read about in school is still alive. I can't believe this.
No he is not.
Jimmy passed away 10 days ago:
https://en.wikipedia.org/wiki/Jimmy_Carter
RIP to him. He really had a long life.
Presidents get great health care and benefits it seems lol
Nice 100 is officially a target, time to switch up and go after a healthy lifestyle.
Any data about the oldests presidents in function?
Jimmy is in God Mode. Let's just say if Trump breaks this record then he'll have a lot more bragging rights than he already does
Must have had a good diet
joe did a great job at that age. I wonder who to blame if a party didn't run country well, the president or the team?
Damn, biden is only 82. Dude seems 95
♦️ You got 0.01 FELT for sharing high vibes on Hive.
📋♦️ FELT Info
Just picked up one of these babies on eBay to power my new miner that is coming next week!
So glad to be getting back in the #mining game! It's what really brought me into #crypto in the first place!
which miner you get?
Goldshell Mini Doge III - Gets 700 MH/s at 400W in full go mode and 550 MH/s at 260W in low power mode. Perfect for a small off-grid solar setup. I can run 3-4 miners on this one PSU.
sounds like a sick setup!
Yeah, next step is to buy the solar panels, charge controller, batteries, and inverter I need. LOL. But it's not that bad. Going to run on grid until I get the solar all built.
sounds like a fun project
Hi, @l337m45732,
This post has been voted on by @darkcloaks because you are an active member of the Darkcloaks gaming community.
Get started with Darkcloaks today, and follow us on Inleo for the latest updates.
How much heat does it put out?
Not sure yet. Wouldn't imagine it would be too bad with the size.
I haven an old miner that uses mining specific GPUs. (nvidia GTX 1060 equivalents). Not useful for mining these days but still ok on Einstein@home. I got a server power supply and breakout board. Sometimes cheaper and a lot more reliable.
Yeah, I thought about getting a mining rig going because I have a couple of older RX580s and 480s that I would at least like to stick on Ravencoin, but not sure if it's worth it these days. Sill might in the future, but I am liking the specs on these DOGE/LTC miners.
are you mining Bitcoin?
Finally, a workout plan that pays off...literally! 😉💪💰

#Hive #Actifit #Crypto #rewards
Oh change of weather ❄️
Nice photo my bro
Thx, the street lights did the most work !LOLZ
lolztoken.com
She laughs while I'm tickling and is angry at me when I stop.
Credit: reddit
$LOLZ on behalf of ben.haase
(5/10)
Delegate Hive Tokens to Farm $LOLZ and earn 110% Rewards. Learn more.@satoshyls, I sent you an
Looks very pretty!
Glad I am not there. 😀
It's still snowing bro? This must feel so cold man
It's keep falling down 😅
when will this thing end 🤣
On #sunday, no worries !LOLZ
lolztoken.com
You re-tire it.
Credit: reddit
$LOLZ on behalf of ben.haase
(2/10)
PLAY & EARN $DOOM
@jetraven, I sent you anamen bro
Pokemon Crystal for the Game Boy Color was one of several very popular Pokemon games for Nintendo's portable systems.
#retrogaming #pokemon #bbh #cent
Check out the original post for more details: https://ecency.com/hive-140217/@darth-azrael/pokemon-crystal-game-boy-color-866c3b78fdb01
https://inleo.io/threads/view/rentmoney/re-leothreads-vpr4syrw
I still have !BEER tips to giveaway. Taking request in the original thread & this threads comment section.
#beer #community #fun #crypto #hiveengine
Oh yes, I like free #beer ! 🍺🍺🍺🍺🍺🍺
Excellent, one is on the way.
!BEER
View or trade
BEER.BEERHey @hirohurl, here is a little bit of from @rentmoney for you. Enjoy it!Learn how to earn FREE BEER each day by staking your
BEER.I would appreciate some!
Coming right up.
!BEER
Thank you man
Cheers,
!BEER
View or trade
BEER.BEERHey @awesomegames007, here is a little bit of from @rentmoney for you. Enjoy it!BEER at dCity game to buy cards to rule the world.Did you know that <a href='https://dcity.io/cityyou can use
View or trade
BEER.BEERHey @awesomegames007, here is a little bit of from @rentmoney for you. Enjoy it!Learn how to earn FREE BEER each day by staking your
BEER.The server is on the way.
!BEER
What's going on with the Hive Engine? Been having issues for the past 12 hours
seems fine on my end? whats wrong?
Can't access my wallet on beeswap, ecency won't load properly and neither will my keychain
Hi, @caspermoeller89,
This post has been voted on by @darkcloaks because you are an active member of the Darkcloaks gaming community.
Get started with Darkcloaks today, and follow us on Inleo for the latest updates.
I'll test mine and see if it works, but I don't have experience with LeoDEX, can I do everything I want to do on Hive engine but will LeoDEX?
Love to hear it!
https://inleo.io/threads/view/katerinaramm/re-khaleelkazi-pmndmhlj
i think I have to try it out myself and see if it gonna work for me
Evel Knievel’s most dangerous stunt in 2025 would be going to Britain & posting #memes. #elonmusk #meme #lolz #cent
Interesting to know that most Greeks think this way. 👀
interesting statistic. Haven’t thought of such a thing until reading this.
Greece is a beautiful country!
In my opinion, everyone thinks their culture is superior to others. At least that's how I feel about it.
A Rich and well documented history.A major key why another group of people would assume themselves more superior than others, who hardly know a thing about there passed making them repeat the same mistakes and not have nothing to build on.
Thinking like this can get such countries in trouble.
Greece, unfortunately the economy isn’t saying the same thanks to centralization and the controlling minority.